

English Summary
2q33.1 Microdeletion Syndrome, also known as Glass Syndrome or SATB2-Associated Syndrome (SAS), is an ultra-rare genetic disorder caused primarily by deletions or mutations in the SATB2 gene. Key features include moderate to severe intellectual disability, profound speech impairment, craniofacial abnormalities (e.g., cleft palate, micrognathia), dental issues, and behavioral challenges such as autism-like traits, aggression, and self-injury. The disorder results from the loss of SATB2 function, which is critical for brain development, bone formation, and genetic regulation. Diagnosis is confirmed through genetic testing, and non-invasive prenatal testing (NIPT) may assist with early detection. There is no cure, but supportive, multidisciplinary care can significantly enhance quality of life. Management strategies include early intervention, speech and motor therapy, behavioral treatment, epilepsy control, and attention to skeletal and dental health.
Alternative Names
- Glass syndrome※
- SATB2-associated syndrome (SAS)
- SATB2-associated syndrome due to a chromosomal rearrangement
※ Glass syndrome is caused by heterozygous interstitial deletions in the chromosome region 2q32-q33. It can also be caused by heterozygous mutations in the SATB2 gene located on 2q33.1, which lies within the chromosomal region of Glass syndrome.
Overview

Glass syndrome is characterized by severe intellectual disability, microcephaly, and craniofacial dysmorphism, and is caused by interstitial deletions at chromosome 2q32.2-q33.1. This syndrome was first reported in 1989. Sixteen years later, four cases were described with delayed development (both physical and mental), unusual facial features, and distinctive behavioral patterns marked by alternating confusion, euphoria, aggression, anxiety, and self-injury.

Four years after that, clinical reports described three individuals with small heterozygous deletions at 2q33.1 affecting only the SATB2 gene. All three shared severe developmental delay, intellectual disability, and dental anomalies, but their other clinical features varied. Two of the three also displayed behavioral abnormalities or mild dysmorphism. This led to the conclusion that SATB2 strongly contributes to some of the features associated with 2q32-q33 deletion syndrome (commonly known as Glass syndrome).
2q33.1 microdeletion syndrome is characterized by intellectual disability of varying severity and craniofacial dysmorphism such as micrognathia (small jaw), downslanting palpebral fissures, cleft palate, and dental crowding. Additional features may include seizures, joint laxity, arachnodactyly (abnormally long, slender fingers and toes), and a happy, sociable disposition.

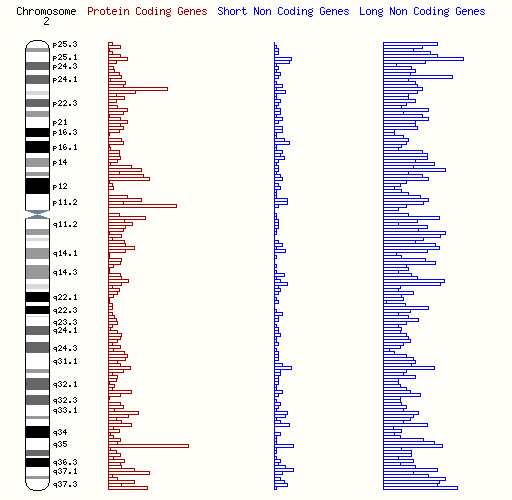
SATB2遺伝子(染色体2q33.1領域に位置)のヘテロ接合型変異が、病気の症状の主な原因であるというThere is strong evidence that heterozygous variants in the SATB2 gene (located in the 2q33.1 region) are the primary cause of the syndrome. However, six other genes are also located in this region: PGAP1, HSPD1, CASP10, TMEM237, ALS2, and BMPR2. Each of these genes has been linked to specific clinical disorders, and some symptoms overlap with or co-occur alongside those described in this article. This is because disruption of normal gene function may also affect neighboring genes.
These genes are typically associated with:
- Hereditary spastic paraplegia (PGAP1, HSPD1)
- SATB2-associated syndrome (SAS) (SATB2)
- Autoimmune lymphoproliferative syndrome (CASP10)
- Joubert syndrome (TMEM237)
- ALS-related disorders, including amyotrophic lateral sclerosis (ALS) (ALS2)
- Hereditary pulmonary arterial hypertension (BMPR2)
When larger deletions spanning 2q32.2–q33 (including but not limited to 2q33.1) occur, symptoms and severity are expected to be more variable.
Studies of patients with different deletions in the 2q33.1 region, and the overlap between genetic variants and clinical symptoms, highlight SATB2 as a key driver of 2q33.1 microdeletion syndrome. This article focuses on SATB2, which contributes to many of the syndrome’s characteristic features.
SATB2-associated syndrome (SAS) is extremely rare, with fewer than 1,000 individuals estimated worldwide.

Cause and Diagnosis
SATB2-associated syndrome results from loss of function of the SATB2 gene, which plays a crucial role in brain development, skeletal formation, and other vital processes. SATB2 regulates DNA architecture and fine-tunes gene expression. When SATB2 is impaired, this regulatory system breaks down, with widespread developmental consequences.
In the brain, SATB2 is especially important for forming connections among specific neurons in the cerebral cortex. These connections are essential for cognition, including learning and memory. Loss of SATB2 disrupts expression of many related genes, affecting brain structure and function. This leads to developmental delay, intellectual disability, and difficulties with speech and language.

SATB2 also regulates genes controlling skeletal development, so dysfunction may cause cleft palate and other bone abnormalities.
In summary, SAS arises because SATB2 acts as a “master regulator” of gene activity. Loss of SATB2 affects multiple interconnected biological systems, leading to the characteristic features of the syndrome.
Advances in DNA sequencing have made non-invasive prenatal testing (NIPT) a reliable and safe screening method. Unlike invasive procedures such as amniotic fluid testing or fetal FISH (fluorescence in situ hybridization), NIPT analyzes fetal DNA fragments in maternal blood, avoiding risk to both mother and fetus while providing accurate results.
Symptoms and Management
SAS is a very rare genetic disorder that affects multiple body systems, causing developmental, physical, and behavioral challenges.
- Developmental delay & intellectual disability: ranging from mild to severe, most often moderate-to-severe.
- Speech impairment: many affected individuals are non-verbal or have extremely limited vocabulary. Gestures, sign language, or augmentative/alternative communication devices are commonly used.
- Motor development: delayed milestones such as walking; hypotonia (low muscle tone) is common.
- Behavioral issues: autism-like traits, hyperactivity, impulsivity, aggression, self-injury, and anxiety. Sleep disturbances and sensory processing difficulties are frequent. Some individuals have a cheerful, friendly personality.
- Neurological features: hypotonia, seizures in ~20% of cases, EEG abnormalities during sleep (sometimes without seizures), and Rett-like repetitive hand movements in rare cases.
- Craniofacial features: long face, high forehead, thin upper lip, micrognathia.
- Palatal anomalies: cleft palate, high-arched palate, bifid uvula; feeding difficulties often begin in infancy.
- Dental problems: abnormal tooth shape, delayed eruption, crowding, frequent damage. Severe feeding difficulties may require feeding therapy or gastrostomy tube placement.
- Skeletal issues: scoliosis, bowed legs, joint stiffness, low bone density with frequent fractures. Growth restriction is common, especially in large deletions including SATB2.
Other features: strabismus, vision problems, congenital heart defects (rare), and urogenital anomalies (e.g., cryptorchidism, hypospadias in males).

Management
- Early intervention with developmental support, speech therapy, and alternative communication tools.
- Physical and occupational therapy to improve motor skills and muscle tone.
- Behavioral therapy and medications (if needed) for hyperactivity, anxiety, or aggression.
- Sleep management with behavioral strategies or medical support.
- Anti-epileptic drugs if seizures occur.
- Surgical and therapeutic interventions for craniofacial anomalies and feeding problems.
- Bone health monitoring and treatment (exercise, calcium/vitamin D, medications for severe cases).
- Regular check-ups: dental, ophthalmologic, bone density, growth monitoring, and evaluations for heart or urogenital anomalies.
A multidisciplinary care team—pediatricians, neurologists, speech therapists, orthopedists, etc.—is essential for optimizing quality of life and developmental potential.

Prognosis
There is currently no cure for SAS. Management focuses on supportive care to improve quality of life, functional abilities, and minimize complications.
Prognosis varies widely, depending on symptom severity. Some individuals live relatively independently with mild symptoms, while others face significant lifelong challenges. As understanding of the molecular basis of SAS improves, so will diagnosis, counseling, and patient care.
Increased awareness and support are expected to further improve quality of life and long-term outcomes for affected individuals.

Further Resources
SATB2 Portal (English, with photos): A comprehensive resource on SAS
Unique (English, with photos): Information sheets on 2q33.1 deletions and 2q31–q33 deletions
Unique (English, with photos): Information sheet on SATB2-associated syndrome (SAS) / Glass syndrome
References
- Wahl, N., Espeso-Gil, S., Chietera, P., Nagel, A., Laighneach, A., Morris, D. W., Rajarajan, P., Akbarian, S., Dechant, G., & Apostolova, G. (2024). SATB2 organizes the 3D genome architecture of cognition in cortical neurons. Molecular Cell, 84(4), 621-639.e9. https://doi.org/10.1016/j.molcel.2023.12.024
- Pradhan, S. J., Reddy, P. C., Smutny, M., Sharma, A., Sako, K., Oak, M. S., Shah, R., Pal, M., Deshpande, O., Dsilva, G., Tang, Y., Mishra, R., Deshpande, G., Giraldez, A. J., Sonawane, M., Heisenberg, C. P., & Galande, S. (2021). Satb2 acts as a gatekeeper for major developmental transitions during early vertebrate embryogenesis. Nature communications, 12(1), 6094. https://doi.org/10.1038/s41467-021-26234-7
- Shimojima Yamamoto, K., Shimomura, R., Shoji, H., & Yamamoto, T. (2024). Glass syndrome derived from chromosomal breakage downstream region of SATB2. Brain and Development, 46(9), 281–285. https://doi.org/10.1016/j.braindev.2024.06.003
- Balasubramanian, M., Smith, K., Basel-Vanagaite, L., Feingold, M. F., Brock, P., Gowans, G. C., Vasudevan, P. C., Cresswell, L., Taylor, E. J., Harris, C. J., Friedman, N., Moran, R., Feret, H., Zackai, E. H., Theisen, A., Rosenfeld, J. A., & Parker, M. J. (2011). Case series: 2q33.1 microdeletion syndrome–further delineation of the phenotype. Journal of Medical Genetics, 48(5), 290–298. https://doi.org/10.1136/jmg.2010.084491
- Van Buggenhout, G., Van Ravenswaaij-Arts, C., Mc Maas, N., Thoelen, R., Vogels, A., Smeets, D., Salden, I., Matthijs, G., Fryns, J.-P., & Vermeesch, J. R. (2005). The del(2)(Q32. 2q33) deletion syndrome defined by clinical and molecular characterization of four patients. European Journal of Medical Genetics, 48(3), 276–289. https://doi.org/10.1016/j.ejmg.2005.05.005
- Rosenfeld, J. A., Ballif, B. C., Lucas, A., Spence, E. J., Powell, C., Aylsworth, A. S., Torchia, B. A., & Shaffer, L. G. (2009). Small deletions of SATB2 cause some of the clinical features of the 2q33.1 microdeletion syndrome. PloS one, 4(8), e6568. https://doi.org/10.1371/journal.pone.0006568
- Zarate YA, Bosanko K, Fish J. SATB2-Associated Syndrome. 2017 Oct 12 [Updated 2024 Jun 20]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK458647/
- Orphanet. SATB2-associated syndrome due to a chromosomal rearrangement. Retrieved from https://www.orpha.net/en/disease/detail/251028
- Online Mendelian Inheritance in Man. (Last updated August 2023 by Hilary J. Vernon). Retreived from https://omim.org/entry/612313
- Perez, G., Barber, G. P., Benet-Pages, A., Casper, J., Clawson, H., Diekhans, M., Fischer, C., Gonzalez, J. N., Hinrichs, A. S., Lee, C. M., Nassar, L. R., Raney, B. J., Speir, M. L., van Baren, M. J., Vaske, C. J., Haussler, D., Kent, W. J., & Haeussler, M. (2024). The UCSC Genome Browser database: 2025 update. Nucleic Acids Research, gkae974. https://doi.org/10.1093/nar/gkae974
- Harrison, P. W., Amode, M. R., Austine-Orimoloye, O., Azov, A. G., Barba, M., Barnes, I., Becker, A., Bennett, R., Berry, A., Bhai, J., Bhurji, S. K., Boddu, S., Branco Lins, P. R., Brooks, L., Budhanuru Ramaraju, S., Campbell, L. I., Carbajo Martinez, M., Charkhchi, M., Chougule, K., … Yates, A. D. (2024). Ensembl 2024. Nucleic Acids Research, 52(D1), D891–D899. https://doi.org/10.1093/nar/gkad1049
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







