
Sources and references
The information in this guide is drawn from the knowledge of approximately 50 people with the 1q21.1 partial duplication .
PubMed (www.ncbi) allows you to search for abstracts and original articles on the Internet by first author name and publication date. nlm.nih.gov/pubmed). If you wish, you can obtain the paper from Unique.
This leaflet also makes use of Unique’s database (Brunettipieri 2008).
Mefford 2008, Aldinger 2009, Brunato 2009, Greenway 2009, Stanciewicz 2010, Unique
1q21.1 duplication is an extremely rare genetic condition in which a small extra piece of one chromosome is found in the body’s cells. Small extra bits increase the risk of learning and developmental difficulties. However, there are large individual differences. People with the 1q21.1 duplication range from asymptomatic to those with developmental delays and health problems.
Genes and chromosomes
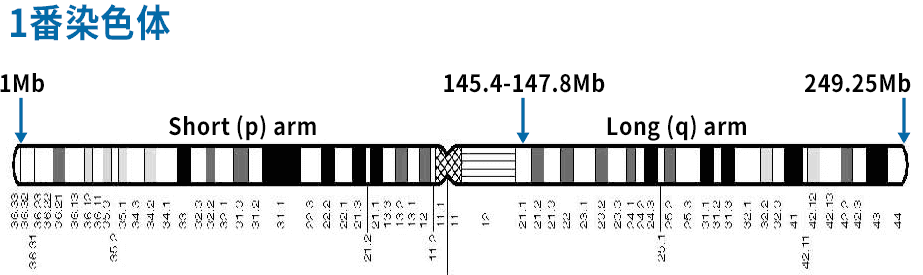
Our bodies are made up of billions of cells. Most cells contain approximately 20,000 genes. Genes act like instructions, directing our growth, development, and body functions. Genes are organized into structures called chromosomes. There are usually 46 chromosomes, and there are two sets of 23 chromosomes: 23 inherited from the mother and 23 inherited from the father. Chromosomes are numbered from 1 to 22, with the exception of the two sex chromosomes (two Xs in girls and one X and Y in boys). Chromosome 1 is the largest chromosome. Each chromosome has a short arm (on the left in the diagram on page 3) and a long arm (on the right), and the short arm is called p, from the French word petit, meaning “small.”
Looking at chromosome 1q
Chromosomes cannot be seen with the naked eye, but when stained and magnified under a microscope, each chromosome has a distinctive pattern of light and dark bands. If you look at the diagram on page 3, you can see that the chromosome bands are numbered outward from the point where the long and short arms meet. In the 1q21.1 partial duplication , the chromosome is broken at two locations in band q21.1, with a small amount of chromosomal material being repeated between them.
When you look at chromosomes under a microscope, you may be able to see where the chromosomes are broken. If there is a large enough extra portion (overlap), you can see a pattern of bands indicating its size.
However, in the case of partial duplication, the extra portion is so small that even a high-powered microscope cannot see it. The extra parts are so small that they cannot be seen even with a powerful microscope and can only be identified using molecular DNA techniques. The most common technology is called microarray (array CGH). Microarrays show minute amounts of DNA on chromosomes. Microarrays can show whether a particular gene or part of a gene is present once, twice, three times, or not at all. Unique publishes a separate guide for array CGH.
Is it a normal genetic variation?
Duplications of 1q21.1 are found in the general population as well as in humans referred for chromosome testing. Initially, these were thought to be part of normal genetic variation between individuals. However, these are more common in people referred for genetic testing and are now thought to increase susceptibility to various developmental disorders.
1q21.1 partial overlap: two sizes
1q21.1 microduplications come in two sizes. The size is around 1 million base pairs. One million sounds sounds like a lot, but it’s actually so small that you couldn’t see it with a microscope. A fragment of about 5 million base pairs is required to be viewed under a microscope. Base pairs are chemicals in DNA that form the ends of the “rungs” of a ladder-like structure. Chromosome 1 is approximately 247 million base pairs. Band 1q21.1 contains 5.4 million base pairs.
bp=1 base pair
kb = 1,000 base pairs
Mb=1 million base pairs
The 1q21.1 duplication is typically located between 146 Mb and 147.8 Mb in the diagram below. This section contains at least nine known genes, and is known to contain many more. Number is a Location on chromosome 1 between 1 Mb (tip of short arm) and position Figure at the bottom of this page 249.25 Mb (tip of long arm) (BrunettiPierri 2008; Mefford 2008)
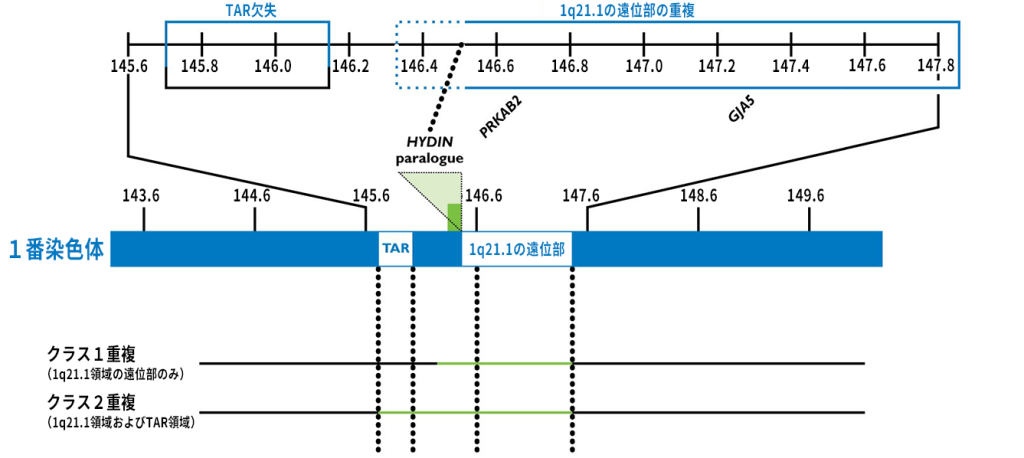
Figure adapted and subsequently updated with kind permission from Dr. Ankita Patel, from Nature Genetics Vol. 40 (12) p1469. Numbers in this figure refer to human genome construct 19 (hg19, see page 4 for details). Your child’s report may point to a different human genome architecture. Contact yourself or a genetics expert.
Helps understand the report.
Size 2 is a larger replica of approximately 1.35-2Mb. This includes 25 known genes. This overlap is from 145.4Mb and 147.8Mb in the diagram below (Brunetti-Pierri 2008; Mefford 2008).
Array CGH Report
The laboratory that discovered the 1q21.1 partial duplication typically sends a report similar to the one below.
arr[hg19]1q21.1(146701190-147623589)x3
Analysis human genome build 19 using microarray technology . This is the reference DNA sequence that the base pair number refers to. Base pairs between 146,701,190 (approximately 146.7 Mb) and 147623589 (approximately 147.6 Mb) are shown to be repeated.
If you take the first long number and the second long number, you get 922399. x3 means there are three copies of these base pairs, rather than the two normally assumed (one on chromosome 1).
arr (RP11-337C18, RP11-533N14, RP11-102F23)x3
Analysis using microarray technology Occasionally, such reports are sent to us when
three markers are found to be repeated and the location of the 1q21.1 band is known .
This report is not very detailed and doesn’t tell you how big the extra portion is.
46,XY,dup(1)(q21.1q21.1)
Number of chromosomes in your child’s cells: 2 sex chromosomes. Males have XY, females have XX There is a duplication or extra material The duplication is from chromosome 1 The chromosome has two breakpoints, both at band 1q21.1. The material between these two branching points is repeated.
Are there people with the 1q21.1 duplication who develop normally and have no health, learning, or behavior problems?
yes, I have. 1q21.1 partial duplication may be silent. Some parents of children with the 1q21.1 duplication may have the same duplication but have no obvious abnormal characteristics or developmental delays. The signs of other parents having a duplicate are so subtle that they are almost imperceptible. Additionally, some children with the 1q21.1 partial duplication develop normally.
The effects of some of these genetic mutations can range from barely noticeable to obvious and severe. In this sense, it can range from mild to severe, like an infectious disease such as influenza. (Brunetti-Pierri 2008; Mefford 2008; Aldinger 2009; Stanciewicz 2010)
Is there a 1q21.1 partial duplication syndrome?
No there is not. The features associated with the 1q21.1 duplication are too diverse to be called a syndrome.
Common situation: both father and son have a partial duplication of 1q21.1 . However, the partial duplication for the father was discovered only after the partial duplication for the son was found.
Most likely characteristics
⦁ Relatively large head
⦁ Increased chance of mild or moderate developmental delay
⦁ Increased chance of autism or autism-like behavior
⦁ Slightly unusual facial appearance
⦁ Heart problems
Other features
⦁ Seizures
⦁ Increased risk of other birth defects
Most likely characteristics
relatively large head

Studies have shown that more than half of people with this partial duplication have large heads, which are large compared to their bodies.
This suggests that partial duplication affects brain growth. People who have this part of chromosome 1 deleted (partial deletion) have very small heads, supporting the idea that the gene in the deleted or duplicated part affects head growth. ing. Genes that appear to be important in determining head growth (see some genes in 1q21.1 on page 19) have been identified.
It has been suggested that there may be a link between small heads and mental health problems, particularly schizophrenia, but this No such relationship has been suggested.
Among the unique members with this partial overlap, the head size is variable. Four of the nine members have large or relatively large heads. Two unique members were born with their skulls already fused together (craniosynostosis). After successful surgery and reconstruction, head growth was average in both cases. Neither child has had seizures.
I ride motorcycles so I always need the biggest helmet.– Adults with 1q21.1 partial duplication
Brain
Of the 27 cases reported in the medical literature, three had structural brain malformations. In one case, the band of nerve fibers connecting the two sides of the brain was thin (callosal hypoplasia), and there was a thin, worm-shaped structure between the sides of the cerebellum, which plays an important role in movement and coordination (cerebellar vermis). The dorsal and bottom regions of the brain were also underdeveloped. One had the cerebellum part of the brain protruding into the spinal canal (Chiari malformation). One case had fluid buildup in the brain (hydrocephalus) (Brunetti-Pierri 2008; Mefford 2008). Endemic members reported no abnormalities in brain structure (endemic).
Increased risk of developmental delays and learning difficulties
Some children with the 1q21.1 duplication develop at a normal rate, cope well academically, and grow into adults who fulfill expected social roles. Others reach developmental milestones later, need additional help in school, and require special schooling. This means that babies and children with partial duplications should be closely monitored to avoid delays, and additional help and treatment should be provided promptly.
The presence of overlap does not predict mild or significant delays or learning difficulties. This spectrum includes people with no noticeable problems and those who are severely affected. Researchers have found that this delay is usually mild or moderate (Mefford 2008; Aldinger 2009; Unique).
Among members of the spectrum, developmental delay ranges from none to severe. Infants and young children may be delayed in reaching developmental milestones (sitting, crawling, and walking), as well as fine motor control, toilet training, and personal care skills (dressing and undressing, self-feeding, and laundry). There is.
Adults who do not appear to be affected by partial duplication may have subtle symptoms.
Excellent manual dexterity.
– 3 years old
A very sloppy writer. He is not good at handling small items.
– Adults with 1q21.1 partial duplication
Increased risk of autism or autism-like behavior
Children and adults with the 1q21.1 duplication are able to be affectionate and socialize without behavioral problems. However, these minorities may be at risk for a range of behavioral disorders and autistic behaviors. However, it is not yet known whether these unusual behaviors are the result of a partial duplication or a chance association of 1q21.1 . In one series in the medical literature, 4 of 8 children were diagnosed with autism and 1 showed challenging behavior; in another series of 24, 2 were diagnosed with autism or had autistic features; one had attention deficit hyperactivity disorder and one had a mood disorder (Brunetti-Pierri 2008; Mefford 2008; Aldinger 2009).
Of the unique members, 3 out of 11 have been diagnosed with autism or an autism spectrum disorder. Other characteristics noted by families include difficulty relating to other children, possibly unpredictable behavior, and apparent behavior towards adults (4 children, 3 year old child, 1 child). This may be due to a child’s physical preferences, he cries and gets tired easily, and his mood improves due to epilepsy (3 years old). The children, who were nearly 6 years old, also exhibited somewhat rigid thinking and behavior, inappropriate friendships, and anxiety. Two children were reported to require a lot of sensory stimulation. One adult reported receiving counseling for “anger issues.”
She is affectionate, likes cuddles and hugs, has a beautiful smile, and is sweet and kind .
– 2 years old
In my everyday life, I am happy and smiling. Because of his sensory processing disorder, on the advice of his occupational therapist, he wears a compression shirt under his arms at school and a compression vest during the day. On the advice of an occupational therapist, he wears a compression shirt under his arms at school.
– 3 years old
He loves making people happy. Even at this age, pleasing people is very important to him. He’s really sweet and can easily switch into cute and kissable moods. He always wants to be held and wants to stroke my hair, so I have to stroke his hair.
– 3 years old
A slightly different look
Most children and adults with the 1q21.1 partial duplication look just like other members of their family. A doctor trained to look for unusual features may notice eyes that are set far apart or a protruding forehead, but these signs are subtle and may not be obvious. In about half of the cases reported in the medical literature, at least slightly unusual facial features are noted. Unique parents also commented that their child has the widest grabella (the space between the eyebrows and above the nose).
Similar to other family members: 2 months [1], prominent eyes that lessen with age [1], small nose [1], prominent cannibal cleft (fold of skin across the inner corner of the eye) [1], wide, flat nasal bridge [1], low-set ears [1] (Brunetti-Pierri 2008; Mefford 2008; Aldinger 2009; Unique).
A photo gallery of adults and children wearing partial duplications has been published (Brunetti-Pierri 2008) and made available by Unique to families who request it.

Beautiful features, no obvious differences.
– 2 years old
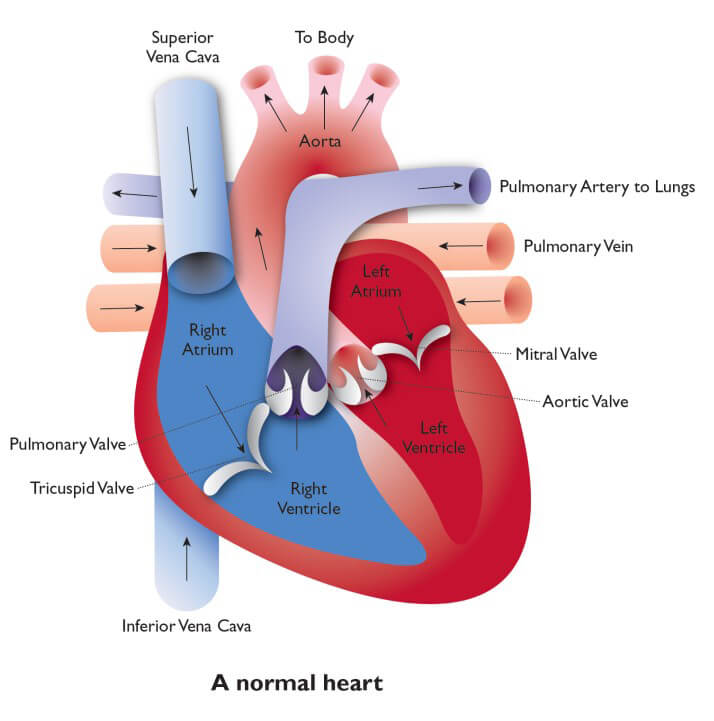
Heart disorder
It is unknown whether having a duplication of 1q21.1 puts a baby at risk for heart problems. Some researchers have found that the number of babies born with structural heart problems is higher than expected, while others disagree. Overall, 4 out of 35 infants were reported in different series in the medical literature. Two of these patients had a ventricular septal defect (VSD, see page 9) and one had a univentricular heart (see page 9) (Brunetti-Pierri 2008; Mefford 2008). Another person reported a partial duplication (see page 3) of the TAR region inherited from his father (Brunei 2009). The patient had complex heart disease including transposition of great vessels, VSD, pulmonary artery stenosis, and right ventricular hypoplasia (see below and page 9).
Among the unique members, 7/31 were born with heart defects, including 3 with VSD, 1 with pulmonary artery stenosis, 1 with pulmonary vein stenosis, and 1 with unspecified spontaneously occluded cardiac foramen. , and one with unspecified chronic heart failure. Two babies were born with tetralogy of Fallot [ToF]. Five of the seven required surgery to correct heart problems (unique).
One study on ToF found that nearly 1 in 100 infants had either a partial duplication (4/512) or deletion (1/512) at 1q21.1 , which would be expected by chance. The proportion was much higher than that of These newborns had heart defects but no cognitive, social, or neurological problems (Greenway 2009). Of the two unique children with ToF, one had moderate to severe developmental delay and the other was too young to be evaluated (unique).
Two genes have been identified that may contribute to heart problems (see Some of the genes on 1q21.1, page 19).
Looking healthy after heart surgery.
– 3 years old
The heart problems diagnosed in individual children may be single or multiple. They are as follows.
Ventricular septal defect (VSD) – A hole in the wall between the two pumping chambers (ventricles) of the heart. This allows blood to flow from the left ventricle to the right ventricle, increasing blood flow to the lungs. Treatment is individualized. Small VSDs may close spontaneously, and larger VSDs usually require surgical repair to prevent lung damage resulting from excessive blood flow.
Transposition of the great arteries : A condition in which the main blood vessels leading from the heart (aorta and pulmonary artery) are reversed. Babies with this condition usually require surgery soon after birth.
Pulmonary artery stenosis : A condition in which the entrance to the artery that supplies blood to the lungs is abnormally narrow. This narrowing usually affects the pulmonary valve and the pulmonary artery itself.
Pulmonary vein stenosis : A problem (blockage) in the blood vessels that return oxygen-rich blood from the lungs to the heart. It may occur in just one pulmonary vein, but more often it occurs in multiple veins at the same time. The cause of the blockage is the thickening of the walls of the vein. Surgery to widen the pulmonary veins is usually a short-term solution.
Tetralogy of Fallot : A complex heart disease involving both a VSD and a subvalvular blockage of the artery leading to the lungs. Blue blood (deoxygenated blood) cannot easily take oxygen into the lungs, and some of it flows through the holes into other pump chambers, from where it is pumped into the body. In the absence of other risk factors, more than 95% of infants with tetralogy of Fallot undergo successful surgery within the first year of life.
Single ventricle heart : means there is one ventricle (lower part of the heart, pumping chamber) instead of two, but in practice this is rare. More generally, the term “univentricular heart” refers to a heart in which blood from the upper two heart chambers [the atria] flows into the dominant right or left lower heart chambers [the ventricles] through poor connections. means. Another way to describe this is as a dual entrance ventricle. Typically, there is non-dominant, underdeveloped second ventricle. Univentricular hearts usually require surgical repair.
Other features
⦁ Seizure
seizures have been reported in 5 of 35 patients in the medical literature and 4 of 11 in unique members. Among the distinctive members, “absenteeism” or seizures began in early to middle childhood. It has been reported to be controlled with standard antiepileptic drugs such as sodium valproate (Brunetti-Pierri 2008; Mefford 2008; Unique).
⦁ Spinal Curvature
One case of spinal curvature (scoliosis) in a series of 24 cases was reported in the medical literature (Brunetti-Pierri 2008). Unique cases have been reported in 4 out of 10 cases, 2 in otherwise healthy adults. A 2-year-old infant developed curvature by 6 months, measured 30 degrees by 2 years, and treated with a back brace.
A teenager developed severe scoliosis after a growth spurt. Two adults reported minor problems.
When I enlisted in the military, my doctor told me that my spine was slightly curved, but this did not interfere with my military service. No big deal.
– Adult
⦁Mild genital anomalies Mild
genital abnormalities were reported in 3 out of 27 cases in the medical literature, including hypospadias (a hole in the underside of the penis instead of the tip) and undescended testicles at birth. has been done. Both of these abnormalities can be corrected surgically (Brunetti-Pierri 2008; Mefford 2008) if necessary. Among the nine cases, one was born with undescended testicles and another had ambiguous genitalia. Both cases required surgery (specific).
⦁ Increased risk of other birth
defects Other mild or more severe birth defects have been observed, but these do not seem to follow a pattern and whether there is a causal relationship with the 1q21.1 duplication is unknown. Reports in the medical literature include: a small sacral depression at the base of the spine [1]; hemivertebrae (incomplete development of one side of the vertebrae, resulting in a wedge shape) [1]; flaccid or dislocated joints [2]; birth These include multiple joint contractures (arthrogryposis [1]; clubfoot [1]; Brunetti-Pierri 2008; Mefford 2008).
At birth
Most unique families report normal pregnancies, with 1 in 9 reporting noticing a lack of fetal movement. At birth, the weight was 2.69 kg (5 lb/15 oz) for infants born at or near birth, in good physical condition at birth, and whose preeclampsia was induced at 35 weeks, and 4.36 kg for term infants. Kyros (9 pounds/10 ounces). Most newborns were healthy, but one born at 35 weeks showed jaundice. Despite having a good birth weight and good Apgar score (a measure of health at birth), she looked and acted like a red-skinned premature baby. She had red skin, slept a lot, woke up to nurse, and struggled to maintain her body temperature.

About feeding
Of the 9 unique members, 5 had no feeding difficulties and were successfully breastfed. One baby who was breastfed remained underweight. One neonate born with craniosynostosis was tube fed for 2 weeks, but was artificially fed by the 3rd week. The baby, who was acting like a premature baby, was weak and lacked the reflex needed to suck.
He woke up every two hours so he could be fed breast milk from a nursing cup. After two weeks, the gaps between nightly feeds became longer. After 7 weeks he had enough strength to start breastfeeding and continued for 2 years. Although he was delayed in drinking from other drinks, he learned to drink from a cup at 2 o’clock. Despite this laborious start, he eventually responded enthusiastically to the solids.
He is a good eater. When he was about 8 months old, we started him on full-fledged diets and he was really into it. He would eat anything and eat a lot. Sometimes he had to say no because he was eating the same amount as his grandma. Now he eats normal amounts and is progressing well.
– Almost 3 years old
One child eats well, but has difficulty handling cutlery and prefers to use his hands, so we needed weighted cutlery. Some children are very picky eaters even at age 6, refusing lumpy foods like fruit yogurt.
Two unique members reported gastroesophageal reflux disease. Gastroesophageal reflux disease is when food backs up in the stomach and can be spit up or inhaled, causing a chest infection known as aspiration pneumonia. One is an adult and the other is a 6-year-old child whose gastric juices come out when they bend over.
Growth
Of the 27 cases reported in the medical literature, growth was normal in 22 cases. Three infants or children experienced failure to thrive, with abnormally slow growth rates, one with uneven growth, and one with advanced bone age (Brunetti-Pierri 2008; Mefford 2008). Of the 9 unique members, the average growth rate was 4, 2 were short, and 1 was slim. Two children are tall and one is thin. Four families commented that their child was underweight or above average weight.
He has a thick frame, and when others pick him up, they say, “You’re so sturdy.”
– 3 years old
If I were to ask if I’m tall or short, or if I’m average, I’d say I’m on the short side, but I’m actually more slender. My head is too big and my arms are a little too short. Other parts of the body are normal. A year or two ago, I looked a little overweight and chubby, but now I’m more proportioned.
– 3 years old
Health and welfare
Infections are common in childhood. Although there is no evidence that children with the 1q21.1 duplication are more susceptible to infections than other children, one family reported that their 3-year-old son caught all the common colds and was exposed to many respiratory illnesses in early childhood . It is reported that he had. In another family, the child suffered from multiple infections, including pneumonia and meningitis, before the child was 2 years old. This family and one other family reported that their health deteriorated rapidly when their children became ill. Two children have asthma or asthma-like symptoms and one has mitochondrial complex IV symptoms and is taking coenzyme Q10. In addition, four people reported skin diseases, one with psoriasis and three with eczema. It is not known whether these symptoms are associated with the 1q21.1 partial duplication. Between illnesses, parents report that their children are healthy, happy, and making progress. (Brunetti-Pierri 2008; Unique)
I think it’s also affecting his respiratory issues. She can’t cough as hard as other children, so the phlegm stays in her lungs.
– 2 years old
Hearing
Ear infections are common in young children, including those with 1q21.1 duplications . In the medical literature (Brunetti-Pierri 2008), it has been reported that 1 in 24 people and 2 in 9 Unique members had tubes (grommets) inserted to equalize pressure on both sides of the eardrum. Neither child had permanent hearing loss, but one had sensory impairment, was hypersensitive to loud sounds, and feared harsh sounds (unique).
Vision
Of the 35 people reported in the medical literature, 4 people have visual impairment, but the type varies. One had rotary nystagmus (involuntary movements of the eyes in a circular motion), one had strabismus, one had cataracts (clouding of the crystalline lens), and one had increased intraocular pressure (glaucoma) (Brunetti-Pierri 2008 ; Mefford 2008). In addition to one adult who realized he was farsighted in his mid-20s, there was also a child who had astigmatism in both eyes and had to observe things in a different position than usual.
He never looked straight at us when he was born or for several months afterwards.He couldn’t follow us with his eyes. At 10 weeks he visited an ophthalmologist, but the cause was not found. The first time I saw our faces was over 5 months ago.
Sleep
5 out of 10 unique members report having some difficulty sleeping. One baby was very difficult to put to sleep for the first four months. One child is very restless and is constantly moving while sleeping, even at the age of 6. One child is difficult to put to sleep and wakes up in the middle of the night, but he uses a sound machine to help him sleep. One child stays awake from 2-3pm to 6am every night. And some children are restless and need little sleep. It is not yet clear whether children with the 1q21.1 duplication have greater sleep problems than other children or whether there is a pattern of sleep problems associated with the duplication (unique).
Study

Among people with 1q21.1 partial duplication who need extra support with learning due to a learning disability, 8 out of 11 say they have at least mild or moderate difficulty (Meford 2008). Unique’s experience reflects this, with a wide range of member abilities. One adult with partial overlap runs his own business and another has a master’s degree. Among children, the effects on learning vary widely. The comments below demonstrate this rich variety.
She has a good memory and learns best with a consistent approach. She looks at the book, but she cannot read yet, and when she picks up the pen she scribbles. – 2 years old
We do not believe he has any learning difficulties or disabilities. He is very good at listening to music and he enjoys singing very much. He can solve a 50-piece puzzle by himself. He doesn’t like playing house or anything that gets his hands dirty like paint. He is into toy cars and real cars and he knows some manufacturers and points them out. He is playing with toy cars and when he sees the wheels spinning he gets very excited. My memory is average and I like learning new things. He doesn’t like to draw, but when he does, he scratches with a pencil. He’s still too young to use computers, but I don’t think he’ll have any problems. He will attend a special school for children with communication and autism problems.
– 3 years old
She has an excellent memory and remembers the lyrics to songs, but sometimes she won’t say her own name. When I pass by a restaurant, I take a bite of what I want to eat or what I ate there, such as hot dogs or chicken. Music is something I’m better at. Honestly, he’s lazy. If he is not interested in what he is learning, he will not participate. He is always “reading” books. He looks at the picture and he chats about the book. He doesn’t like drawing or coloring. He is interested in computers, but not keyboards. He puts his hand on the adult mouse and clicks the button. He attends a special education kindergarten and receives learning support from a special education teacher.
– 3 years old
She can count to ten but can’t read. She can write her name. She likes using computers at school. Although she participates in a language program at a mainstream school, she does not have a statement of special educational needs.
– 5 and a half years old
Communication

In the medical literature, there have been reports of 3 out of 24 cases of delayed language abilities in children with partial duplication of 1q21.1 (Brunetti-Pierri 2008). Among the unique members, speech and language delay is a consistent finding, even in adults who show only very subtle signs that may be due to segmental duplication. Frequent themes are better understood than the ability to express them verbally, and the speech of the language lacks clarity. Some children were initially able to communicate their needs successfully in sign language, spoke in mid-childhood, and developed fluid speech in adolescence. Students may also receive education in speech and language units, focusing on communication skills.
The following description is exemplary.
Communicate aloud.
– 5 months
They communicate through sign language, gestures, pointing, pulling, and sounds, but it is difficult for them to understand all sounds.
– 2 years and 5 months old
I try to speak, but sometimes the meaning is not clear. There is a problem between what you think with your brain and what you say with your mouth. According to tests conducted by speech therapists, he understands more than he can tell us or explain clearly. That’s why we often use questions with “yes” or “no” answers. For the past six months, we’ve been using hand signals and emojis. He gets sad and sometimes angry if you don’t understand what he wants to say. His speaking voice is very soft and slurred, and when I ask him to repeat something, he goes completely silent. He speaks his first words around his first birthday and now uses 2-3 word phrases, but many words sound the same. – 3 years old
They use their hands to communicate, such as holding hands and touching things they want. At the age of two and a half, she began using words to express what she wanted using one word. Now I use phrases of one to three words, but most of the sounds are unclear. I talk a lot, but no one understands me.
– 3 years old
Strangers have a hard time understanding her. She is expressive but not receptive.
– 5 and a half years old
I didn’t have speech therapy, but I was a little slow in starting to speak. For a long time I was pointing out everything I wanted.
– Adults with 1q21.1 partial duplication
It is too early to know whether this partial overlap will have a consistent effect on locomotor ability, but at this point it does not appear to be the case. In families where a parent is found to have partial duplication after the child is diagnosed, the parent’s mobility is usually unaffected, even if the child’s mobility is delayed. Children with 1q21.1 duplication
who have developmental delays may need additional support to achieve “baby” milestones such as sitting and moving around. Low muscle tone (hypotonia). Children benefit from physical therapy, and all children benefit from regular graded exercises to increase muscle strength and agility. Among the unique members with developmental delays, infants learned to roll over between 5 and 10 months. They learned to sit between 6 and 16 months, to move (shuffling, creeping, crawling) between 7 and 20 months, and to walk between 13 and 60 months. Children climbed the stairs between 18 months and 1 year. 3 years
When I first sat down, I couldn’t sit straight and sat a bit like a pudding. Crawling was very slow due to limited torso rotation. By her first birthday, she was sliding by bumping and bouncing on her butt.This continued until he was able to walk around 23 months. Now he has become a normal child, almost 3 years old. It takes a little while for him to turn around as his torso rotation is still limited. There’s also the issue of balance. The physical therapist believes that he falls often because his body proportions are slightly atypical (he has a large head and short arms). His arms have limited mobility, so when he falls, he has a hard time getting back on his feet and often ends up falling on his face. When he walks long distances he uses a special buggy. The buggy is built so that you can sit up straight, and you wear a helmet so you don’t hurt if you fall.
– 2 years old
I have a sensory processing disorder, so I’m always moving and jumping.I love climbing and swinging.
– 3 years old
She moves quickly, trips and falls often, and is anxious about using the stairs.
– Almost 6 years old
Why are people with the 1q21.1 duplication so different from each other?
We still don’t get this right. People with different sizes of overlap for which no consistent differences have yet been detected
can have very different characteristics than people with the same size of overlap in the same family.
One reason for the uncertainty is that the 1q21.1 band of chromosome 1 has such a complex structure that its exact DNA sequence has not been completely mapped. There are still 15 gaps on the map, and these gaps may contain genes that contribute to the effects of partial duplication. Additionally, there may be important genetic and environmental factors that we do not yet understand.
Why investigate partial duplication of 1q21.1?

Most babies and children are tested because their pediatrician or specialist suspects they have a chromosomal problem.
The 1q21.1 partial duplication may explain the symptoms or may be considered unrelated. The impact of this overlap will not be known until more people are diagnosed.
Among Unique’s members were two babies who were investigated for craniosynostosis (premature fusion of some of the bony plates that form the skull). In one case, subsequent development was unaffected and the craniosynostosis was not considered to be due to segmental duplication. In the other case, the contribution of the 1q21.1 partial duplication is unknown. One child developed seizures at the age of 6 years. Four of the children had developmental disabilities, and one had unusual facial features. The other had spinal curvature and she developed seizures at 18 months. The other was very lame at her birth, but there were no problems with her heart. Four of the seven people inherited the partial duplication from their father or mother, who previously did not think they had an abnormality in their chromosomes.
How did this happen?
The 1q21.1 duplication can occur suddenly for no apparent reason or can be inherited from either the mother or father. The only way to be sure is to check the parents’ chromosomes. Checking the parents’ chromosomes is also necessary even if the parents themselves are perfectly healthy and do not have any developmental problems.
If either parent has the same partial duplication, it is almost certainly inherited.
If both parents have normal chromosomes, the 1q21.1 duplication is a new occurrence. In genetic terms, this is called de novo (dn). The new 1q21.1 partial duplication was caused by a mistake that occurred when the parents’ sperm or egg cells were formed, or very early after fertilization. As a parent, you cannot change or control this.
In other words, there is nothing the parents did before or during pregnancy that would cause a partial duplication.
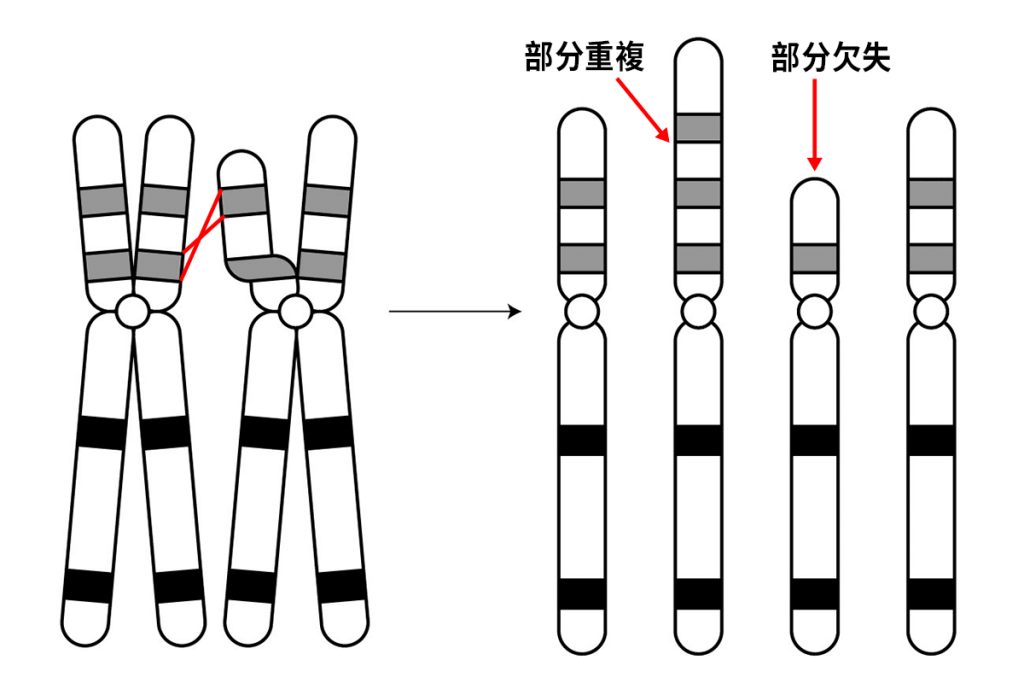
At one point in the development of the egg and sperm cell, all the chromosomes, including the two chromosomes 1, pair and exchange segments. To ensure precise pairing and equality of exchanged fragments, each chromosome “recognizes” matched or nearly matched DNA sequences on the other chromosome. However, many DNA sequences are similar across chromosomes, and it is thought that mismatches can occur. The result is unequal swapping, resulting in deletions or duplications.
The 1q21.1 region has a very complex structure. Three-quarters of them consist of at least four blocks of DNA that are more than 90% similar to each other. It is very likely that these very similar blocks caused the mismatch. When the researchers looked at the breakpoints in individual human chromosomes, they found that they were located within these nearly identical DNA sequences. In most people, the cut points occur in approximately the same area.
If one member of a family with a 1q21.1 duplication is mildly affected, are other members of the same family also mildly affected?
Not necessarily. There are many differences between members of the same family.
We know that if one person is mildly ill, others can be severely ill and clearly affected.
Will it happen again?
If both parents have normal chromosomes, it is unlikely that a child will have a 1q21.1 duplication or other chromosomal abnormalities . In rare cases (less than 1%), the 1q21.1 duplication may be present in some of the egg cells or sperm cells of both parents, even though both parents have normal chromosomes in blood tests . This is called germline mosaicism , and means that parents with normal chromosomes in a blood test can have multiple children with duplicate parts.
Families in which the 1q21.1 duplication is inherited from both parents have a 50% chance of having a child (girl or boy) with the 1q21.1 duplication in a single pregnancy . However, the effects of the 1q21.1 partial duplication on child development, health, and behavior cannot be predicted with certainty.
At the Genetics Center, you can receive counseling before trying to get pregnant again.
Is my child with the 1q21.1 partial duplication similarly affected?
Children with a partial duplication of 1q21.1 may wish to have children. Although this condition has not been known long enough to know if it affects fertility, fertility may be normal. In each pregnancy, the duplicate has a 50% risk of inheriting it and a 50% chance of having a non-duplicate child.
It is very likely that one’s ability to care for children is closely related to one’s own learning ability.

Part of the 1q21.1 gene
The part of 1q21.1, which is duplicated in most people, is rich in genes.
GJA5 is a gene that produces a protein known as Connexin40. It is expressed in the upper ventricles (atria) of the heart, and not having enough of it is associated with congenital heart disease. However, some people without this gene have normal hearts, and the reason for this is not completely understood (Christiansen 2004; Mefford 2008; Brunet 2009).
PRKAB2 is another gene expressed in the heart (Brunet 2009).
The HYD1N gene, found on chromosome 16q22.2, has a partial copy that was inserted into 1q21.1 during evolution. The HYD1N gene on 1q21.1 is active only in the brain.
Individuals with the deletion have a small head size, while individuals with the extra gene have a large head size. This strongly suggests that the HYD1N gene plays a role in determining head size (Brunetti-Pierri 2008; Mefford 2008).
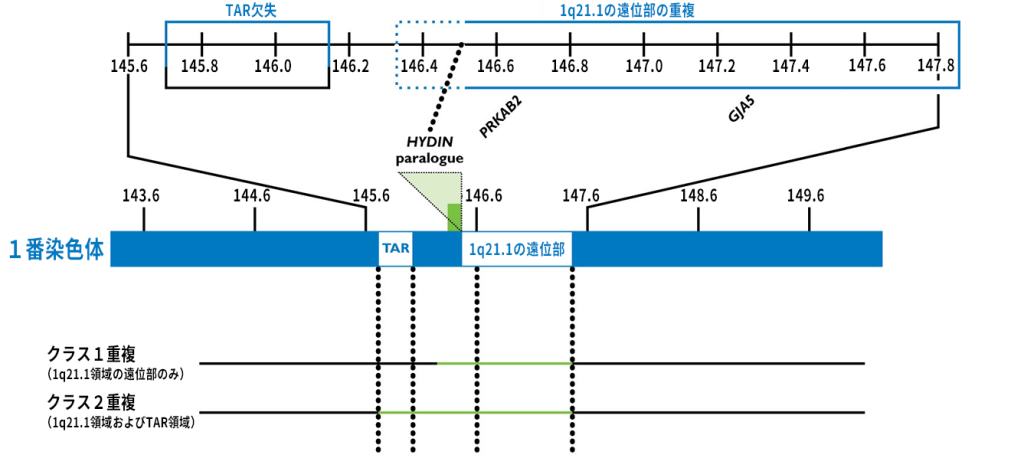
Figure adapted and subsequently updated with kind permission from Dr. Ankita Patel, from Nature Genetics Vol. 40 (12) p1469. Numbers in this figure refer to human genome construct 19 (hg19, see page 4 for details). Your child’s report may point to a different human genome architecture. Contact yourself or a genetics expert.
Please help us understand the report.

Support and information
Rare Chromosome Disorders Support Group
The Stables, Station Rd West, Oxted, Surrey. UK RH8 9EE
Phone: +44(0)1883 723356
info@rarechromo.org I www.rarechromo.org
There is a Facebook (www.facebook.com) group for families affected by 1q21.1 duplications , called 1q21.1 partial deletions and duplications.
Join Unique for family links, information and support.
Unique is a charity that receives no government funding and relies entirely on donations and grants. If you would like to help, please donate via our website: www.rarechromo.org/donate.
Thank you for your cooperation of everybody.
At Unique, we refer to other organizations’ message boards and websites to help families looking for information. This does not mean that we endorse or are responsible for their content.
This guide is not a substitute for personal medical advice. Families should consult a medically qualified clinician regarding all matters related to genetic diagnosis, management, and health. We believe this information to be the best available at the time of publication and are provided by Dr. Heather Mefford, Assistant Professor of Pediatrics, Department of Medical Genetics, University of Washington, USA, and Marge, Professor of Reproductive Genetics, University of Warwick, Unique’s Chief Medical Advisor.・Reviewed by Professor Hulten (2010).
2010 Version 1.0 (PM)
2011 Version 1.1 (PM)
2013 Version 1.2 (SW)
Copyright © Unique 2018
Rare Chromosomal Disorders Support Group Charity Number 1110661
Registered in England and Wales Company Number 5460413
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







