
Alessandra Di Nora1 , Germana Lena1 , Andrea June1 , Alessia Di Mari2 , Pierluigi Smirari3 , Carmelo Minardi4 , Piero Pavone3
1 Department of Pediatrics, Postgraduate Training Program, Clinical and Experimental Medicine, University of Catania, Italy
2 Department of Radiology, Postgraduate Training Program, Department of Radiology, University of Catania, University of Catania, Italy
3 Department of Pediatric Neurology, University of Catania , Italy
4 Department of Pediatric Neurology, University of Catania, Italy University Hospital “G. Rodolico” Department of Anesthesia and Intensive Care
Global Med Genet
Correspondence address:
Dr. Alessandra Di Nora, Hospital Polyclinic, SanoMarco, University of Catania, Via S. Sofia 78, 95123 Catania, Italy
(email: alessandradinora@gmail.com)
Summary
Diagnosis is difficult in children with developmental delays and neurological disorders due to the wide range of causes. From the past decade, the use of array comparative genomic hybridization (CGH) has provided a major contribution to obtaining diagnosis of complex phenotypes. Chromosome 7 is of interest in medical genetics because it is frequently associated with chromosomal aberrations, rearrangements, and deletions, including clinical symptoms . Here, we report a 3-year-old boy with severe neurodevelopmental delay, craniofacial dysmorphia, and pulmonary stenosis. This array CGH analysis revealed a 14.4 Mb duplication on chromosome 7 (7q21.3-7q31.1) . By reviewing the literature to date, the authors report for the first time a previously unreported neurological and dysmorphic malformation associated with this rearrangement.
Keywords
7q21.3-q31.1, serial CGH, onset delay, facial features, duplication
Introduction
Individuals with duplicate long arms (q) have been rarely reported. Isolated “pure” 7q types are classified by chromosomal abnormalities that involve either the entire long arm or the interstitial, proximal, or distal portions of the chromosome segment. 1 , 2 , 18 Novales et al. 14 differentiated affected individuals according to chromosome 7q segments and found the following results: Individuals with interstitial duplications of 7q22 to 7q31 exhibit facial features consisting of a frontal protuberance, long eyelashes, narrow cleft palate, eyebrows, hirsutism, small nose, long upper lip, ocular defects, and are associated with skeletal abnormalities, cleft palate, and premature death. Not accompanied by. Individuals with a 7q31 to 7qter duplication exhibit developmental delays, including facial features such as a large fontanelle, narrow cleft palate, hirsutism, small nose, cleft palate, micrognathia, and low-set, malformed ears. , skeletal abnormalities and early death were also recorded. The 7q32 to 7ter duplication was characterized by developmental delay, small nose, and low-set ears, without micrognathia or cleft palate, and was associated with skeletal abnormalities, neurological symptoms, and early death.
In this paper, we report a 3-year-old boy with a pure partial duplication of the long arm of chromosome 7 spanning 14.4 Mb from 7q21.3 to q31.1. We report the clinical symptoms observed in this case and compare them with the clinical features of children with distal segment involvement, as well as with those of children with interstitial chromosome 7 segment involvement. The purpose of this comparison is to clarify possible clinical symptoms specific to each affected segment.
Case presentation
This 3-year-old male patient is a healthy, third child of unrelated Italian parents. The two siblings (a 5-year-old sister and a 7-year-old brother) are healthy and have no family history of genetic disorders . At the time of his pregnancy, his mother was 32 years old and his father 35 years old. Her mother denies having any infections during pregnancy, and she has never smoked or taken any medication during pregnancy. Intrauterine ultrasound showed developmental stricture by 7 months, and the mother noted decreased fetal movements. The child was delivered by caesarean section at 39 weeks of gestation due to breech position. Birth weight was 2,350 g (3rd percentile), length 48 cm (10th percentile), and occipitofrontal circumference (OFC) 33 cm (3rd percentile). On the second day of life, the child suffered from respiratory distress and was admitted to the neonatal intensive care unit of the Pediatric Clinic of the University of Catania, Italy, for treatment and examination.
Head ultrasound showed mild hypodensity of the periventricular white matter. Echocardiography showed pulmonary valve stenosis with an atrial septal defect. On day 10 of life, the patient was discharged from the hospital in good condition without indication for immediate cardiac intervention. During the first month, the patient’s clinical picture was mainly characterized by minor facial features and delayed developmental milestones, especially regarding hypotonia. At 2.5 years of age, the child was admitted to the Department of Pediatrics of the University of Catania, Italy, for evaluation for developmental delay and craniofacial anomalies. At this age, weight was 12 kg (10th percentile), length 88 cm (10th percentile), and OFC 47 cm (3rd percentile). According to “Morphological elements: standard terminology: Am J Med Genet 2009, 149A (1): 1-127”: microcephaly, tarry encephalopathy, prominent frontal protuberance, arched eyebrows with shaved medial area. , from the medial superior corner folds, downward facing palpebral fissures, flat nasal bridge, thin, flat filter of the nose with a rounded tip and anteverted nostrils, thin lips, low recessed ears with axes of rotation, and thin hairs. It showed craniofacial features.
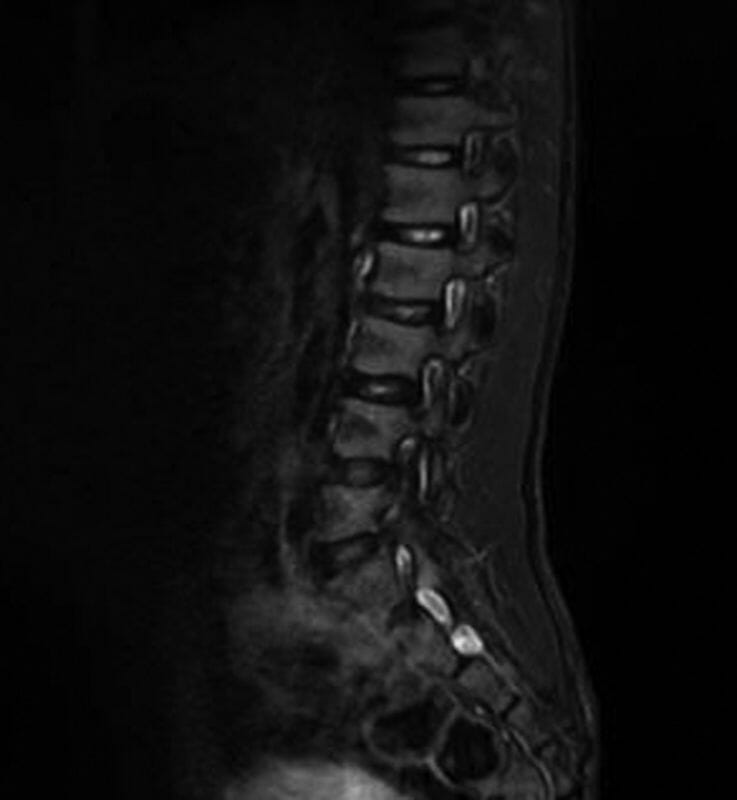
The sarcoma was hypotonic and the subcutaneous tissue was poor. The patient presented with ankle valve stenosis, knee in joint contracture, keel chest, scapular wing, wrist laxity, and rectus abdominis diastasis. He was developmentally delayed and was able to say very heavy words. His gait was unsteady. Osteonecrosis of the patella and loss of reflexes are ineligible. Systolic mouse 2/6 Levine was marked, and echocardiography confirmed the presence of pulmonary valve stenosis with an atrial septal defect. Routine laboratory analysis of electrolytes, plasma and urinary amino acids, thyroid markers, organic acids, plasma purines, and transferrin isoelectric focusing revealed left cryptorchidism, and total cholesterol was within normal limits. EEG during wakefulness and sleep were normal. Brain magnetic resonance imaging (MRI) using a diffusion-weighted imaging sequence showed regular volumes and anatomy of infratentorial and supratentorial structures and ventricles. Spinal MRI revealed a cleft in the posterior arch of S5, lipomatosis of the distal sacrum from S3 to S5, and a small Tarlov type periapical cyst in the right S2 ( see Figures 1 and 2 ).
Figure 1 Spinal magnetic resonance image showing S5 posterior arch cleft and lipomatosis of the distal sacrum.

Figure 2 Spin magnetic resonance imaging showing an S2 periapical cyst.
Genetic testing
According to the International System for Human Cytogenetic Nomenclature11 , high-precision karyotype analysis performed after lymphocyte culture in children and their parents has an average resolution of 550 bands, and molecular cytogenetics A cell-applied probe was used.
Array comparative genomic hybridization (CGH) (human DNA, Promega) analysis using Cytofure ISCA 8×60K v.2 (Protein O-GicNacTransferase, OGT) was performed on medonogenes extracted from peripheral blood samples from children and their parents. I did tick DNA. Software analysis was performed with Cytofure Analysis Software (University of California, Santa Cruz, Genome Assembly 19). The quality score (Derivative Log Ratio Spread, DLRS) was <0.25. Analysis parameters: 4 consecutive probes. Resolution: 50~100Kb. A next generation sequencing (NGS) panel of RASopathies was performed.
Result
Analysis showed a 46,XY karyotype in the child with an intrachromosomal partial duplication of the long arm of chromosome 7, 14.4Mb (7q21.3-q31.1):arr[hg 18] (hereinafter Figures 3A, 3B ). The centromeric margin of duplication is made up of the normal oligomer at position 95054968 pb and the duplicate oligomer at position 109476740 pb. Telomeric margin created by a normal oligomer of 109557905 bp and an overlapping oligomer of 109476740 bp ( Figure 4 ). RASopathies NGS analysis showed no changes. Karyotype and array CGH of both parents were normal.
Figure 3 (A,B) Caryotype of a child showing intrachromosomal partial duplication on the long arm of chromosome 7
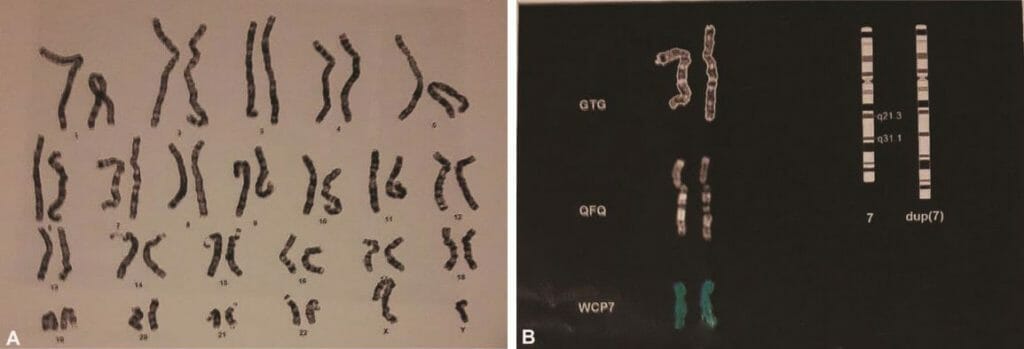
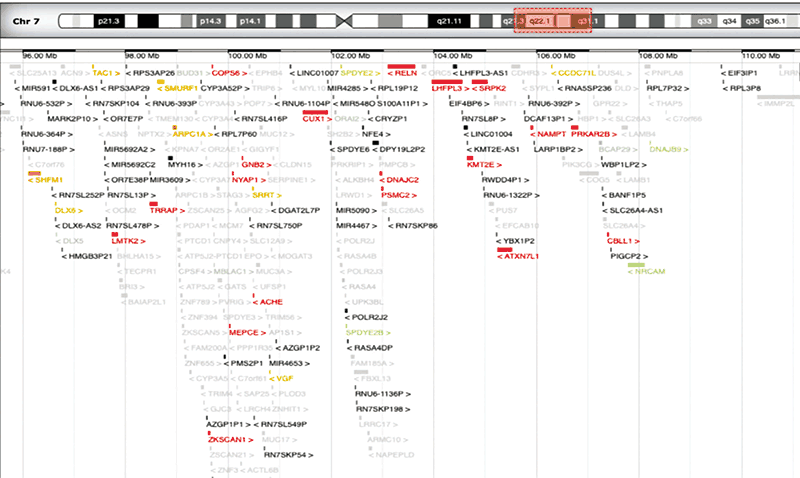
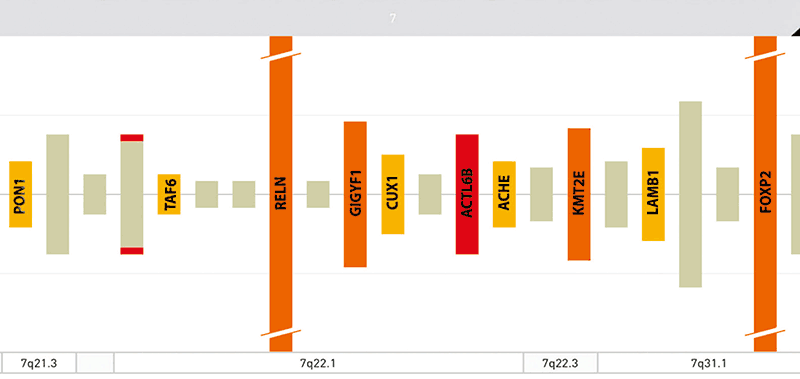
Figure 4 Imaging modified from OMIM showing genes included in the reconstructed region
Consideration
The child exhibited a complex of congenital anomalies consisting of mild nonspecific craniofacial features, microcephaly, mild developmental delay, and cardiac and skeletal defects. The genitals, hands, and abdomen were also affected. Congenital heart disease consisted of pulmonic valve stenosis with septal defect, skeletal abnormalities showed S5 posterior arch fissure, S3-S5 distal sacral lipomatosis, and right S2 periapical cyst Tarlov type; joint contractures. and knee in ankle valve stenosis were also present. Additionally, rectus abdominis diastasis, left cryptorchidism, and wrist laxity were observed. Array CGH revealed a large genomic duplication of 14.4 Mb on chromosome 7q21.q31.1 with several OMIM and RefSeq genes : the rearranged region contains more than 230 genes ( Figure 4 ). According to the SFARI gene database, some such as ACTL6B, FOXP2, PONI, KMT2E are involved in synaptic plasticity and autistic signaling mechanisms as well as other structures responsible for congenital diseases affecting the brain and other organs. It is involved in physical abnormalities ( Fig. 5 ).
Figure 5. Image of modified SFARI gene showing genes involved in autism spectrum disorder.
Chromosome 7q is susceptible to different structural rearrangements. Attempts to highlight specific clinical signs depending on the involved stromal, proximal, or distal segments have not been clearly defined. Alfonsi et al. compared the clinical characteristics of an observed case presenting with a partial chromosome 7q duplication involving the q21.1-q22.3 region with six patients from the literature with similar 7q rearrangements. I tried. These authors found intellectual retardation and the presence of low-set malformed ears in all cases, including their own, strabismus and frontal features in 6 cases, and skeletal abnormalities in 5 cases. Three of the patients exhibited several similar craniofacial features such as genital defects, macrocephaly, and high eyelids, small upturned nose, retrognathia, cleft palate, and high arched palate. . 1 The authors concluded that patients with pure chromosome 7q proximal fragments did not develop specific diagnostic clinical features. 1 In this study, we analyzed the clinical data of each of the 8 cases of the 7q duplication interstitial (7q22-7q32) segment reported in the literature, including this case, and evaluated clinical similarities or differences ( Table 1 ) . . In the interstitial group, 3 males and 4 females were affected, with no gender-specific prevalence. Developmental delay and mild nonspecific facies were reported in all cases. In particular, looking at some facial features, frontal prominence and epicanus were reported in 6 out of 7 cases, low-set ears in 4 cases, and retrognathia in 2 cases. Hypotension and growth retardation were observed in 6 of 7 cases, and intraocular strabismus was observed in 5 cases. Three children had microcephaly, and abnormal cardiac, skeletal, and genital sweating was reported in this case but not in the other children. Hirushutism and hip subluxation were reported in one case, and brain malformation and renal dysplasia were only in one case. 2 , 4 , 7 , 15 , 17 , 18 , 21 Analysis of these results reveals that, with the exception of intellectual retardation and mild craniofacial delay, no specific clinical signs indicating a clear diagnosis were raised. be.
Table 1 Comparison of clinical data of 8 cases with pure 7q distal duplications 1 , 3 , 6-10 and the present case with pure 7q stromal duplication
| distal 7q | current case | |
|---|---|---|
| gender | M/F: 7/1 | M |
| facial features | 8/8 | + |
| large head | 5/8 | – |
| Occurrence delay | 8/8 | + |
| autism spectrum disorder | 1/8 | – |
| skeletal abnormality | 4/8 | + |
| genitourinary malformations | 2/8 | + |
| congenital heart disease | 1/8 | + |
We reviewed clinical data for pure interstitial 7q duplications and pure interstitial 7q duplications , comparing 6 cases reported in the literature with 6 cases currently observed in children ( Table 2 ). 3 , 6 , 10 , 17 , 20 , 22 Analysis of these results suggests that few nonspecific craniofacial features, intellectual delay, and a small frequency of skeletal disorders are associated with distal and interstitial chromosome 7q. It seems clear that infiltration is the most typical clinical sign in any of the current groups of children.
Table 2 Clinical data of six reported cases (cases 8, 11-15) and pure interstitial 7q duplication of the present case
| Grace et al. (1972) | Berger et al. (1974) | Serville et al. (1975) | Rome et al. (1990) | Megalbane et al. (2000) | Weimer et al. (2011) | current case | total | |
|---|---|---|---|---|---|---|---|---|
| chromosome 7 | q22-q32 | q21-q31 | q22-q31 | q22-q31.2 | q22-q31.3 | q21.1-q31.3 | q21.3-q31.1 | |
| sex | F | M | M | F | F | F | M | 3M/4F |
| facial features | ||||||||
| Front boss processing | – | + | + | + | + | + | + | 6/7 |
| epicanthus | + | + | + | + | + | + | + | 6/7 |
| Postmicrognathia | – | – | – | – | + | – | + | 2/7 |
| bass | + | – | + | – | + | – | + | 4/7 |
| Development delay | + | + | + | + | + | + | + | 7/7 |
| cerebellopathy | – | – | – | – | + | + | + | 3/7 |
| Low blood pressure | – | + | + | + | + | + | + | 6/7 |
| developmental delay | + | – | + | + | + | + | + | 6/7 |
| congenital heart disease | – | – | – | – | – | – | + | 1/7 |
| genital malformation | – | – | – | – | – | – | + | 1/7 |
| skeletal abnormality | – | – | – | – | – | – | + | 1/7 |
| eye abnormality | – | + | + | + | + | + | – | 5/7 |
| Other abnormalities | – | + | + | + | + | + | + | 5/7 |
Note: Other abnormalities include hirsutism reported in 2 cases (14, 15), hearing loss and renal dysplasia reported in 1 case 8, and spinal abnormalities reported in the present case. .
F Female. M Male.
Note: Other abnormalities include hirsutism reported in 2 cases (14, 15), hearing loss and renal dysplasia reported in 1 case 8, and spinal abnormalities reported in the present case. .
Except for pure isolated 7q chromosome duplications , 7q aberrations can occur in association with rearrangements involving the same chromosome or other chromosomes, leading to different and more complex clinical symptoms. Fruhmesser et al. reported a case of partial trisomy of 7q22q32 with an additional inversion of 7q31.2.2q32.3 . Fifteen children presented with congenital heart disease presenting with developmental delay, failure to thrive, hand abnormalities, patent ductus arteriosus and patent foramen ovale.
Craniofacial features consisted of a frontal protuberance, slightly downward-pointing palpebral fissures, wide nasal root, long affine micrognathia, and prominent ears. Pathtinige et al. reported minimal loss of genetic material on chromosome 14 in girls with trisomy 7q22.-qter. 13 Intrauterine growth retardation, developmental retardation, and ventriculomegaly are associated with craniofacial syndromes that present with asymmetrical cranium, triangular facial shape, high cephalopathy, hypercephaly, frontal lobe, flat nasal bridge, micrognathia, and low-set malformed ears. It was the main symptom with characteristics. 16 The authors agreed with the results in the literature that no clear genotype-phenotype correlation was observed in this case.
The patient presented with a congenital heart defect consisting of pulmonary valve stenosis, an abnormality reported as one of the classic manifestations of Noonan syndrome . This syndrome is associated with alterations involving the RAS/MAPK pathway, as it belongs to a group of diseases called RASopathies that share a common dysregulation of the RAS/MAPK pathway . Due to the current common clinical manifestations in children, including cardiac defects, we expanded our genetic studies using an NGS panel for RASopathy key genes, with negative results in this case. Furthermore, the patient exhibited abnormalities affecting the skeletal system, particularly the spine with S5 posterior arch fissure, sacrococcygeal lipomatosis, and sacrococcygeal malformation. The abnormality (the last one) is part of Currarino syndrome (CS).
CS, known as autosomal dominant sacral agenesis, is a classic triad characterized by partial loss of the sacrum, with damage to the first sacral vertebra, presacral mass, and anorectal anomaly. 18 CS can have a variety of clinical manifestations, ranging from malformations of the tail alone to complex organ system malformations. The disease is associated with deleterious variants in HLXB9, a homeobox gene mapped to chromosome 7q368 . Pavone et al. reported that a female infant presenting with prenatal and postnatal growth retardation and complex malformations with microcephaly, lack of cortical thickening, lower vermis hypoplasia, signs of CS, sacral segmental agenesis and complete coccygeal agenesis. reported that it was observed as intrasacral dermoid, intradural lipoma, ectopic anus, and tethered cord. Children 19-22 showed a de novo duplication of 7q34-q35 and an 8.8-Mb deletion of 7q36. This sequence includes the HLXB9 (CS) gene, and no case report of Pavone et al. was found. 14 A clinical relationship between the spinal malformations reported in this child and those reported in CS has not yet been established.
Conclusion
In conclusion, the clinical signs and body organs observed in individuals involving different proximal, interstitial, and distal pure segments of Q7 duplication are nonspecific and diagnostically unsuggestive. Similar results were obtained for one case with involvement of the involved interstitial segment, except that the unique facial appearance and mild developmental delay nonspecific diagnostic signs were not reported.
Ethical approval
This study complied with the ethical guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the University Hospital “Policrino Gaspéa Rodrico” in Catania, Italy (nd: 1268 23/04/2017). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author ContributionsEach
author has made a substantial contribution to the conception or design of the work and revised it critically for important intellectual content. Furthermore, each author approved the final version to be published. Conversely, each author has agreed to be accountable for all aspects of the work in ensuring that questions regarding the accuracy or integrity of any part of the work are appropriately investigated and resolved. .
No funding
.
No conflicts of interest
declared.
Acknowledgments
Thank you for participating in the survey and agreeing to publish your materials and images.
References
1 Alfonsi M, Palka C, Morizio E, et al. A new case of pure partial 7q duplication. Cytogenetic Genome Research 2012;136(01):1-5
2 Bartsch O, Kalbe U, Ngo TK, Lettau R, Schwinger E. Clinical diagnosis of partial duplication 7q. Am J Med Genet 1990;37 (02):254–257
3 Berger R, Deller J, Ortiz MA. The length of chromosome 7 has fewer trisomies. Nouv Presse Med 1974;3(29):1801–1804
4 CouzinDA,HaitesN,Watt JL, JohnstonAW. Partial trisomy 7(q32–qter) syndrome in two children. JMed Genet 1986;23(05):461-465
5 Fruhmesser A, ErdelM, DubaHC, et al.CombinedDup(7)(q22.1q32.2), Inv(7)(q31.31q31.33), and Ins(7;19)(q22.1;p13.2p13 .2) is a 12-year-old boy with developmental delay and various abnormalities. Eur J Med Genet 2013;56(07):383–388
6 Grace E, Sutherland GR, Bain AD. Familial insertional translocations. Lancet 1972;2(7770):231
7 Keith CG, Webb GC, Rogers JG. Lateral rectus muscle defect associated with duplication of chromosome segment 7q32–q34. J Med Genet 1988;25(02):122-125
8 Kim IS, Oh SY, Choi SJ, et al. Clinical and genetic analysis of the HLXB9 gene in Korean patients with Kararino syndrome J Hum Genet 2007;52(08):698-701
9 Lynch SA, Wang Y, Strachan T, Burn J, Lindsay S. Autosomal dominant sacral agenesis: Currarino syndrome. J Med Genet 2000;37(08):561-566
10 Mégarbané A, Gosset P, Souraty N, et al. Chromosome 7q22-q31 duplication: new case report and review. Am J Med Genet 2000;95(02):164–168
11 Mcgowan-Jordan J, Simons A, Schmid M, eds. ISCN 2016: International System for Human Cell Genome Nomenclature. Basel: S. Karger; 2016
12 NovalesMA, Fernandez-Novoa C, Hevia A, San Martin V, Galera H. Partial trisomy for the long armof chromosome 7. Case report and review. Hum Genet 1982;62(04):378-381
13 Paththinige CS, Sirisena ND, Kariyawasam UGIU, et al. Children with multiple birth defects due to partial trisomy 7q22.1! QTER resulting from maternally inherited balanced translocations: case report and literature review. BMC Med Genomics 2018;11(01):44
14 Pavone P, Ruggieri M, Lombardo I, et al. Currarino triad with microencephaly, sensorineural hearing loss, and distal 7q duplication deletion. Eur J Pediatr 2010;169(04):475–481
15 Pavone P, Corsello G, Marino SD, RuggieriM, Falsaperla R. 7q31.32 partial duplication: first report of a child with deformity, autism spectrum disorder, moderate intellectual disability, and epilepsy. Literature review. Epilepsy Research 2019;158:106223
16 Roberts AE, Allanson JE, Tartaglia M, Gelb BD. Noonan syndrome. Lancet 2013;381(9863):333-342
17 Romain DR, Cairney H, Stewart D, et al. Three cases of partial trisomy 7q due to a rare structural rearrangement of chromosome 7. J Med Genet 1990;27(02):109-113
18 Scelsa B, Bedeschi FM, Guerneri S, Larta F, Introvini P. Partial trisomy of 7q: case report and literature review. J Child Neurol 2008;23(05):572–579
19 Schubbert S, Shannon K, Bollag G. Highly active Ras in developmental disorders and cancer.Nat Rev Cancer 2007;7(04):295-308
20 Serville F, Broustet A, Sandler B, Bourdeau MJ, Leloup M. Trisomy 7q party cell Ann Genet 1975;18(01):67-70
21 Verma RS, Conte RA, Pitter JH. Tandem duplication of the terminal band of the long arm of chromosome 7 (douplication (7)(q36-qter)). J Med Genet 1992;29(05):344-345
22 Weimer J, Heidemann S, von Kaisenberg CS, et al. Trisomy 7q21.2-31.31 was isolated as a result of a complex familial rearrangement involving chromosomes 7, 9, and 10. Mol Cytogenet 2011;4:28
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







