
Erin E. Salo-Mullen, MS, MPH, CGC, Patricio B. Lynn, MD, Lu Wang, MD, PhD, Michael Walsh, MD, Anuradha Gopalan, MD, Jinru Shia, MD, Christina Tran, BS, Fung Ying Man , MD, MSc,Sean McBride, MD, MPH, Mark Schattner, MD,Liying Zhang, MD, PhD,Martin R. Weiser, MD,and Zsofia K. Stadler, MD
School of Medicine, Memorial Sloan Kettering Cancer Center, 1275 York Average, New York, NY, 10065
Surgery, Memorial Sloan Kettering Cancer Center, 1275 York Average, New York, NY, 10065
Pathology, Memorial Sloan Kettering Cancer Center, 1275 York Average, New York, New York, 10065
Radiation Oncology, Memorial Sloan Kettering Cancer Center, 1275 York Ave., New York, NY 10065
Weill Cornell Medical College, 1300 York Ave, New York, NY 10065 New York, NY 10065
Summary
Lynch syndrome is an autosomal dominant disease caused by pathogenic mutations in DNA mismatch repair (MMR) genes. Although commonly associated with clinical features such as intellectual disability and birth defects, adjacent gene deletions can also cause cancer predisposition syndromes. We report a 52-year-old man with Lynch syndrome caused by a deletion of chromosome 2p16.3-p21 . The patient had intellectual disability and presented with prostatic adenocarcinoma with an incidentally identified synchronous sigmoid colon adenocarcinoma exhibiting MMR deficiency with lack of MSH2 and MSH6 protein expression. His family history was not clear. Physical examination revealed short stature, microencephaly with a short forehead and short thumb, brachydactyly, transverse palmar creases, and wide, small feet with plantar hyperpigmentation. The patient underwent total colectomy with ileorectal anastomosis for pT3N1 sigmoid adenocarcinoma. Germline genetic testing of the MSH2, MSH6, and EPCAM genes revealed a complete gene deletion . SNP array-based DNA copy number analysis identified a 4.8 Mb deletion at 2p16.3-p21. In addition to the three Lynch syndrome-related genes, the deleted chromosome segments encompassed NRXN1, CRIPT, CALM2, FBXO11, LHCGR, MCFD2, TTC7A, EPAS1, PRKCE, and 15 genes. Congenital gene defects have been reported in other inherited cancer predisposition syndromes, such as familial adenomatous polyposis . Our report and review of the literature suggest that contiguous gene deletions within the 2p16-p21 chromosomal region are a rare cause of Lynch syndrome, but present distinct phenotypic features, leading to recognition and recognition of this syndrome entity. emphasize the need for
Co-author: Zsofia K. Stadler, MD, 1275 York Ave. Box 295, New York, NY 10065, stadlerz@mskcc.org, Telephone:
646-888-4039, FAX: 646-888-4051
*Co-author
Conflict of Interest: Nothing
Keyword
Lynch syndrome; chromosomal deletion ; prostate cancer, colorectal cancer, 2p
Introduction
Lynch syndrome is an autosomal dominant disease caused by pathogenic mutations in DNA mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2) and deletion of the 3′ exon of the EPCAM (TACSTD1) gene. It is associated with an increased risk of cancer, endometrial cancer, ovarian cancer, gastric cancer, and upper urinary tract cancer [ 1 ]. MSH2, MSH6, and EPCAM genes are located on chromosome 2p. The diagnostic process for Lynch syndrome includes tumor immunohistochemistry (IHC) staining for MMR protein expression, microsatellite instability (MSI) analysis, and germline genetic testing [ 1 ].
Contiguous gene deletion syndromes result from the deletion from a particular chromosomal segment . Contiguous gene deletions have been identified in patients with various clinical features such as intellectual disability, developmental delay, and congenital anomalies [ 2 ]. Many flanking gene deletions are the result of de novo events, as the associated phenotypes are often complex and lead to reduced reproductive fitness [ 2 ].
Although previously reported, adjacent gene deletions are a rare cause of cancer predisposition syndromes [ 3 ]. Here we report a patient with Lynch syndrome caused by a contiguous gene deletion on chromosome 2p16.3-p21 encompassing the MSH2, MSH6, and EPCAM genes. Together with a review of previous reports, we highlight the need to recognize adjacent gene deletion syndromes as underlying causes of developmental abnormalities and the need to consider cancer risk and management of affected individuals according to age. do.
Method
Clinical picture
A 52-year-old man with a history of intellectual disability of unknown etiology was diagnosed with Gleason 7 prostate adenocarcinoma by biopsy after PSA screening of 22 ng/mL. Bone scan was negative. He was scheduled for external beam radiation therapy, but it was not performed due to non-compliance with residual radiation therapy. Upon presentation to our hospital for surgical management, the patient’s caregiver reported a 1-month history of bright red blood per rectum. Preoperative evaluation Whole body and prostate magnetic resonance imaging (MRI) revealed concentric thickening of the distal sigmoid colon, suggestive of a primary tumor and focal prostatic disease. Flexible sigmoidoscopy identified a large partially circumferential nonobstructive mass in the sigmoid colon, and biopsy confirmed an invasive poorly differentiated carcinoma. IHC staining for MMR protein showed the absence of MSH6. Staging CT of the chest, abdomen, and pelvis showed no evidence of distant metastases.
Based on the abnormal MMR IHC results, the patient was referred to the Clinical Genetics Service. A four-generation pedigree did not reveal cancer, colon polyps, or developmental disorders. The patient has no children. Three brothers and two sisters are in their 40s and 50s. My mom and dad are both alive and well in their 70s. Sympathy was denied. The family is of African American descent. Birth with intellectual disability. Language understanding is limited to simple commands, and linguistic expression is limited to a small number of words. He lives with his parents and asks for help with all self-care activities. He attends a daily adult program and requires daily supervision and support. Physical examination reveals short stature (4’8′), microencephaly with a short forehead and short thumb, brachydactyly, palmar transverse folds, fleshy pads on the fingertips, and wide, small feet with plantar hyperpigmentation. ( Figure 1a ). Written informed consent was obtained from the patient’s parent/guardian and the photograph was used for publication.
Genetic evaluation
Based on the presence of MMR deficiency in the colon tumor, the possibility of Lynch syndrome was raised. A possible link between Lynch syndrome and prostate cancer was also pointed out. The patient’s mother provided informed consent for germline genetic testing of the MSH6, MSH2, and EPCAM genes and germline DNA specimens were obtained. Germline genetic testing of MSH6, MSH2, and EPCAM genes was performed at the MSK Diagnostic Molecular Genetics Laboratory (sequencing and multiplex ligation-dependent probe amplification). Following the initial test results, the patient’s mother provided additional informed consent for SNP array-based DNA copy number analysis (Affymetrix CytoScan HD Assay) performed at the MSK Clinical Cytogenetics Laboratory.
Genetic test results
Genetic testing revealed a complete heterozygous genetic deletion of the MSH6, MSH2, and EPCAM genes. Based on this finding, we performed SNP array-based DNA copy number analysis and identified a 4.8 Mb deletion at 2p16.3-p21. In addition to the three Lynch syndrome-related genes, the deleted chromosome section contains the following 24 genes: PRKCE, EPAS1, TMEMAS247, ATPV1E2, HORQ, PIGF, CRIPT, SOCS5, LOC38948, LOC100134259, MCFD2, TTC7A , C2orf61, CLM2, MIR559, KCNK12, FBXO11, FOXN2, PPP1R21, STON1, GTF2A1L, LHCGR, FSHR, and NRXN1 ( Figure 1b ).
Clinical sequencer
A diagnosis of Lynch syndrome was made based on the initial finding of a complete genetic deletion of the MSH6, MSH2, and EPCAM genes. Considering the high risk of metachronous colorectal cancer and the difficulty in complying with bowel preparation for colonoscopy, the option of total colectomy with ileorectal anastomosis was discussed. , was accepted by the family after considering the risks and benefits of various surgical approaches.
He underwent total robotic colectomy with partial rectal resection and mid-ileal rectal anastomosis. Surgical pathology confirmed pT3N1M0 poorly differentiated rectosigmoid adenocarcinoma with lymphovascular invasion and increased tumor-infiltrating lymphocytes; 2 of 42 lymph nodes positive for disease Met. A separate tubulovillous adenoma with intramucosal carcinoma was also observed. IHC staining showed no expression of MSH2 and MSH6 proteins, but normal expression of MLH1 and PMS2 proteins ( Fig. 2a-d ). The patient had an uneventful surgical recovery and received adjuvant chemotherapy including capecitabine and oxaliplatin (CAPEOX). Chemotherapy was stopped early due to cumulative side effects including thrombocytopenia and anemia.
The patient ultimately underwent retropubic radical prostatectomy with nerve-sparing bilateral lymph node dissection. Pathology revealed a pT3a multicentric Gleason 7 (3+4) invasive adenocarcinoma with 5 benign lymph nodes. IHC staining showed no MSH2 and MSH6 protein expression, but MLH1 and PMS2 protein expression was normal ( Fig. 2e-h ).
During follow-up clinical genetic counseling, it was discussed that the contiguous gene deletion was presumed to be responsible for both the patient’s intellectual disability and Lynch syndrome. Furthermore, considering that MSH2 and MSH6 protein expression is not observed in either colon cancer or prostate cancer, both cancers are caused by Lynch syndrome. Although the identified flanking gene deletion is likely of de novo origin, an individualized genetic risk assessment was recommended for the patient’s first-degree relatives.
Consideration
Prior contiguous gene deletions have been reported in the setting of hereditary cancer predisposition syndromes, such as familial adenomatous polyposis [ 4 , 5 ]. Our report describes an adult man with a history of intellectual disability and a new concurrent cancer diagnosis who was found to have Lynch syndrome as a result of a contiguous gene deletion . From a review of the literature, a small number of individuals with similar deletions encompassing 2p16p21 have already been described. [ 6,7,8,9,10 ] ( Figure 1c , Table 1 ) The physical characteristics and level of intellectual disability of our patients were similar to previous reports of individuals with the 2p16.2p21 deletion . However, the patient is the oldest affected individual to be described.
A review of the genes involved in the 4.8 Mb deletion revealed that many genes had potential medical significance ( Table 2 ). Mutations in the EPAS1, MCFD2, and CALM2 genes have been reported to be associated with polycythemia family type 4, combined factor V and factor VIII deficiency, and Long-QT syndrome, respectively. Our patient presented with normochromic normocytic anemia likely due to chronic kidney disease with normal erythropoietin levels, but no evidence of polycythemia familial type 4. Electrocardiogram did not show long QT syndrome. We hypothesize that genotype-phenotype mechanisms may explain why patients do not develop these conditions. Polycythemia familial type 4 is associated with activation as opposed to deleterious mutations in EPAS1 (HGNC ID #3374). Similarly, described alterations in the MCFD2 and CALM2 genes include splice site, frameshift and missense mutations, but not loss of function (HGNC ID # 18451 and 1445, respectively). Previously described patients with 2p16p21 deletions also experienced developmental delay/intellectual disability, and at least two genes, CRIPT and NRXN1, found to be deleted in our patient are associated with central nervous system defects. Given that this patient has a history of intellectual disability, it is likely that this patient’s history of intellectual disability is related to the identified adjacent gene deletion . Of note, the deletion identified in our patient resulted in deletion of 27 genes , but did not include the SIX3 gene. Some previous reports have pointed out that SIX3 is associated with holoprosencephaly.
Regarding Lynch syndrome, this case also highlights the importance of informed decision-making regarding surgical management considering the risk of metachronous colorectal cancer. In a cohort of 50 subjects with MMR gene mutations, Parry et al. No metachronous cancers were found, whereas 74 of the 332 mutation carriers who underwent segmentectomy had metachronous colorectal cancers [11] . In this case, the family’s decision to proceed with total colectomy included considerations of future cancer risk, ongoing need for annual colonoscopies, and quality of life. Another point exemplified by this case is the association between prostate cancer and Lynch syndrome. Although conflicting data exist, a study by Raymond et al. Compared with the general population, the overall hazard ratio for prostate cancer in Lynch syndrome mutation carriers was calculated to be 1.99 (95% CI, 1.31–3.03; P = 0.0013) [12] . Indeed, immunohistochemical staining for DNA mismatch repair proteins in the patient’s prostate cancer tissue revealed deletions in MSH2 and MSH6 proteins suggesting that the Lynch syndrome gene deletion plays a role in the patient’s prostate cancer development. revealed. Finally, only MSH6 protein was absent in the patient’s initial rectosigmoid adenocarcinoma biopsy, whereas the reported retention of MSH2 in the biopsy specimen is likely due to technical issues such as edge artifacts. it is conceivable that. MMR IHC analysis of the patient’s rectosigmoid adenocarcinoma resection specimen lacked both MSH2 and MSH6 proteins, reflecting the patient-identified gene deletion .
The authors’ report of a contiguous gene deletion on chromosome 2p16.3-p21 showed strong similarities to previously reported cases. The etiology of this patient’s intellectual disability has not been previously investigated. More recently developed techniques have provided the ability to detect interstitial chromosomal deletions , which were not available when patients were children. The identified adjacent gene deletion syndrome provides a possible explanation for the patient’s intellectual disability, dysmorphic features, and cancer diagnosis. As children with developmental delays, intellectual disabilities, and birth defects are evaluated using advanced genetic techniques, it is likely that additional cases of chromosomal rearrangements involving cancer predisposition genes will be identified. It is important for healthcare providers, patients and their caregivers to be aware of the associated cancer risks in the setting of such a diagnosis, so that they can be advised at appropriate ages, intensive cancer surveillance, and preventive treatment. , and appropriate medical management such as chemoprophylaxis can be considered.
Acknowledgment
This study was funded in part by the Romeo Milio Lynch Syndrome Foundation, the Kate and Robert Niehaus Clinical Genetics Initiative, and NIH/NCI Cancer Center Support Grant P30 CA008748.
References
1. Lynch HT, Lynch PM, Lanspa SJ, Snyder CL, Lynch JF, Boland CR. Review of Lynch syndrome: history, molecular genetics, screening, differential diagnosis, and medical outcomes. Clin Genet 2009; 76(1):1–18.
2. Nussbaum, RL., McInnes, RR., Williard, HF. Thompson and Thompson Genetics in Medicine. 6.Saunders/Elsevier; Philadelphia: 2004. p. 164-165.
3.Adams SA, Coppinger J, Saitta SC, Stroud T, Kandamurugu M, Fan Z, Ballif BC, Shaffer LG,Bejjani BA. Impact of initial diagnosis of genotype: aCGH-induced microdeletion and microduplication syndromes with cancer predisposition. detection. Genet Med. 2009; 11(5):314–322. [PubMed:19365269]
4.Herrera L, Kakati S, Gibas L, Pietrzak K, Sandberg AA. Gardner syndrome in a man with a 5q interstitial deletion Am J Med Genet. 1986; 25(3):473–476. [PubMed: 3789010]
5.Raedle J, Friedl W, Engels H, Koenig R, Trojan J, Zeuzem S. A de novo chromosome delletementation of chromosome q5 causes familial adenomatous polyposis, dysmorphia, and mild mental retardation. Am JGastroenterol. 2001; 96(10):3016–3020. [PubMed: 11693343]
6.Petit P, Fryns JP. Interstitial deletion 2p with marker chromosome formation is accompanied by the formation of deleted segments, resulting in a stable acentric marker chromosome. Jennette Koons 1997; 8(4):341-343.[PubMed: 9457505]
7.Sanders SR, Dawson AJ, Vust A, Hryshko M, Tomiuk M, Riordan D, Prasad C. Interstitial deletion of chromosome 2p16.2p21. Cringesmorphol. 2003; 12(3):183–185. [PubMed: 14564157]
8. Lucci-Cordisco E, Zollino M, Baglioni S, Mancuso I, Lecce R, Gurrieri F, Crucitti A, Papi L, NeriG, Genuardi M. Novel microdeletion syndrome and hereditary nonpolyposis with loss of the MSH2 locus. Colorectal cancer. Clin Genet 2004; 67(2):178–182.
9.Collins DL, Schimke RN. Cancer predisposition detected by CHG arrays. Genet Med.2011; 13(11):982. [PubMed: 22051689]
10.Morton, SA (Adams), Coppinger, J., Ballif, BC., Shaffer, LG., Ellison, JW., Saitta, SC., Stroud, T.,Manickam, K., Fan, Z. Response to the letter by Collins and Schimke. Genet Med. 2011; 13(11):982–983. [PubMed: 22051689]
11.Parry S, Win AK, Parry B, Macrae FA, Gurrin LC, Church JM, Baron JA, Giles GG, Leggett BA,Winship I, Lipton L, Young GP, Young JP, Lodge CJ, Southey MC, Newcomb PA, Le Marchand L,Haile RW, Lindor NM, Gallinger S, Hopper JL, Jenkins MA. Risk of metachronous colorectal cancer for mismatch repair gene mutation carriers: Benefits of more extensive colon surgery. Gastrointestinal Tract 2011; 60(7):950-957. [PubMed: 21193451]
12. Raymond VM, Mukherjee B, Wang F, Huang SC, Stoffel EM, Kastrinos F, Syngal S, Cooney KA,Gruber SB. Increased risk of prostate cancer in men with Lynch syndrome. J Clin Oncol. 2013;31(14):1713–1718. [PubMed: 23530095]
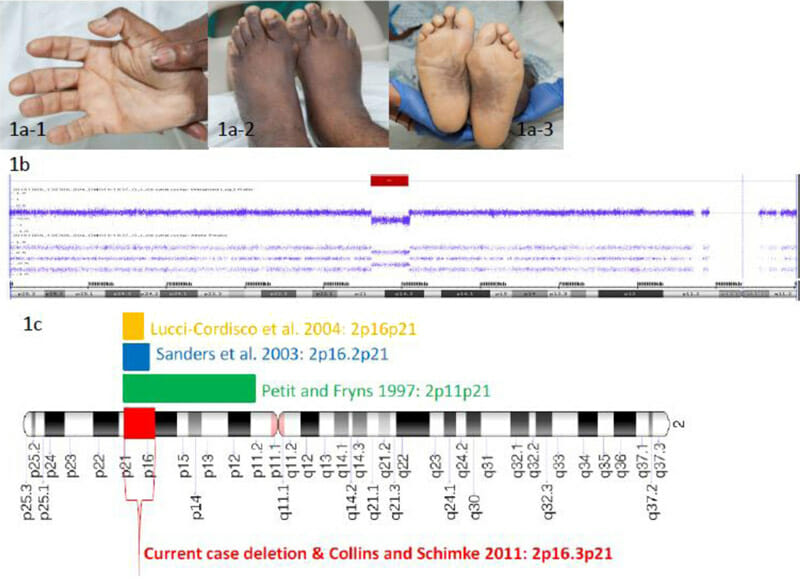
Figure 1 1a ) Brachydactyly of fingers and toes ( 1a-1 and 1a-2 ), palmar transverse folds ( 1a-1 ), broad small feet with plantar hyperpigmentation ( 1a-3 )
1b ) chromosomes Photograph of the proband showing DNA copy number (log2 ratio) and allelic peak profile across the p-arm of 2, red bar indicates stromal deletion (~4.8 Mb) at 2p16.3-p21.
1c ) Animation of chromosome 2 showing sequential gene deletions identified in previously reported cases.
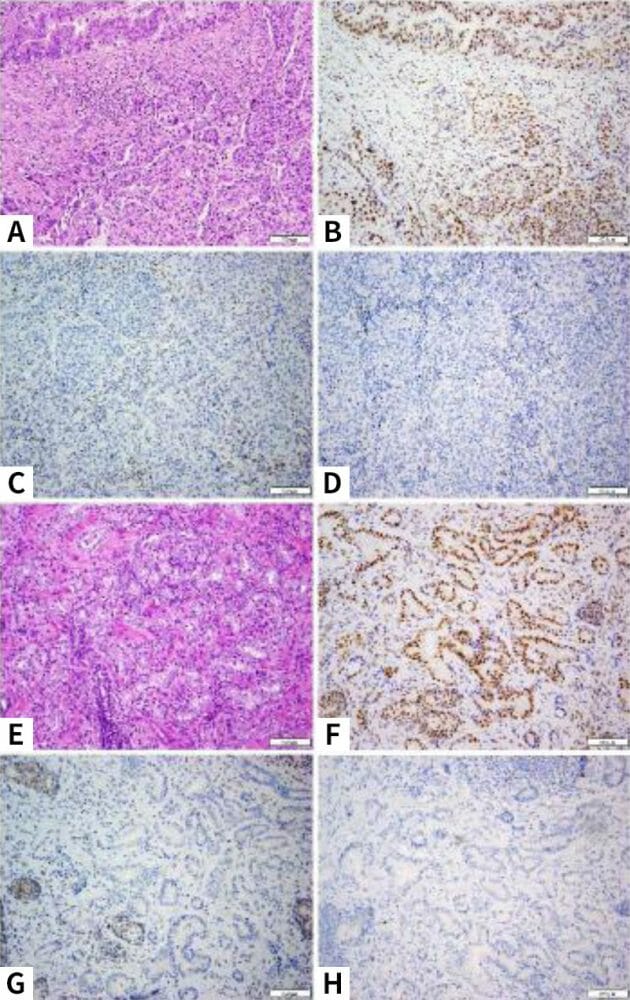
Figure 2 Patient’s colorectal adenocarcinoma (a, H&E) shows a mixed histological pattern with glandular components (top left) and solid components. On immunohistochemistry, the tumor shows the presence of nuclear staining for PMS2 (b) and MLH1 (not shown), but no staining for MSH2 (c) and MSH6 (d). Histologically, the patient’s prostate adenocarcinoma shows typical acinar units (e, H&E). On immunohistochemical examination, this prostate cancer also shows the presence of nuclear staining for PMS2 (f) and MLH1 (not shown), but no staining for MSH2 (g) and MSH6 (h).
Table 1 Reported examples of deletions involving the 2p16p21 region
| reference | delete | Phenotype description |
|---|---|---|
| Petit and Fryns 1997 | 2p11p21+aseful | Mild dysmorphia and moderate mental retardation |
| Saunders et al. 2003 | 2p16.2p21 | Atrial septal defect, mild peripheral impairment, prominent nasal bridge, long smooth neutrophils, mild developmental delay. |
| Lucci-Cordisco et al. 2004 | 2p16p21 | Developmental retardation, precocious puberty, short stature, close skull with narrow forehead, large horizontal eyes with thick eyebrows, prominent columella with nostril hypoplasia, short thumb, simple ears, hirsutism, general obesity, short fingers. syndrome, skin syndactyly between the second and third toes on both sides, moderate mental retardation, colon adenocarcinoma (37 years old) |
| collins sink 2011 | 2p16.3p21 | Developmental delay, mental retardation, short stature, microcephaly, hypocephaly, essentially normal colonoscopy at age 21 (only inflammatory pseudopolyps identified) |
| Morton et al. 2011 | 17.6 Mb (SIX3, MSH2, and MSH6) | Fetus with holocencephaly |
| Morton et al. 2011 | 192 kb (MSH6 and FBX011) | Characteristics of developmental delay and morphological abnormalities |
| Morton et al. 2011 | 537 kb (MSH6 and FBX011) | Characteristics of developmental delay and morphological abnormalities |
| Current report | 2p16.3p21(4.8Mb) | Intellectual disability, short stature, brachycephaly with narrow forehead and short thumbs, brachydactyly, wide small feet with plantar hyperpigmentation |
Table 2 Specific genes with potential medical significance for current patients
| deleted gene | HGNC (HUGO Gene Nomenclature Committee) ID number | Associated phenotype | Phenotypes expressed in current patients |
|---|---|---|---|
| EPAS1 | 3374 | Polycythemia familial type 4 (usually associated with activating mutations) | none |
| CRIPT | 14312 | Postnatal growth restriction, microcephaly, facial dysmorphia, eye abnormalities, developmental delay, recurrent infections, central nervous system defects | Postnatal growth failure, dysmorphic facies, eye abnormalities, developmental delay, central nervous system defects |
| MCFD2 | 18451 | Factor V and factor VIII complex deficiency | none |
| TTC7A | 19750 | Early-onset inflammatory bowel disease and intestinal obstruction | none |
| CALM2 | 1445 | Long QT syndrome | none |
| EPCAM, MSH2, MSH6 | 1152973257329 | Lynch syndrome | Lynch syndrome colon and prostate cancer |
| LHCGR | 6585 | Male secondary sexual development disorder | Our service is not evaluated. |
| NRXN1 | 8008 | Pitt-Hopkins-like syndrome 2 | Intellectual disability, psychomotor delays, language limitations, communication and social difficulties, thin eyebrows, prominent nose, wide mouth, thick ears, lots of smiling, laughing, and waving, and being happy and excited. Easy-going attitude, strabismus, short stature, small hands and feet, flat feet, abnormally thick fingers and toes |
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







