
Duplication of 14q
Chromosome 14 duplication is a rare condition that occurs when an extra piece of genetic material arises from one of the body’s 46 chromosomes, resulting in an extra copy of the gene present on that piece. The correct amount of genetic material is required for normal growth and development. Extra genetic material is likely to cause several problems. However, the nature of the problem depends on the cloned chromosome fragment, the genes it carries and, in some cases, the parent of origin. To date, more than 730 genes have been identified on chromosome 14.
Genes and Chromosomes
Our bodies are made up of billions of cells. Most cells have a complete set of tens of thousands of genes. Genes act like a set of instructions that control growth and development and how the body works.
Genes have minute thread-like structures called chromosomes. There are usually 46 chromosomes, 23 inherited from the mother and 23 from the father. Therefore, we refer to two sets of 23 chromosomes as a “pair.” With the exception of the two sex chromosomes (two X chromosomes for girls, one X chromosome for boys, and one Y chromosome for boys), chromosomes are numbered from 1 to 22 and are generally the largest. becomes the minimum from
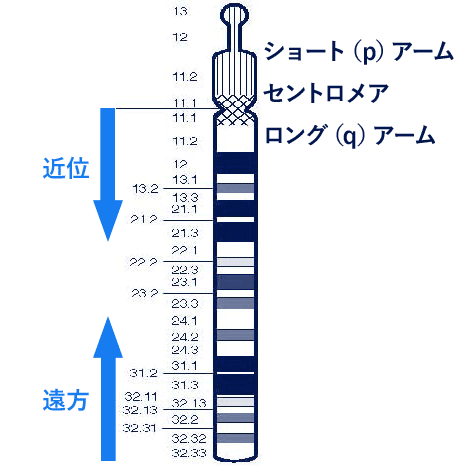
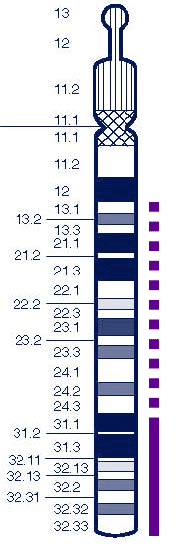
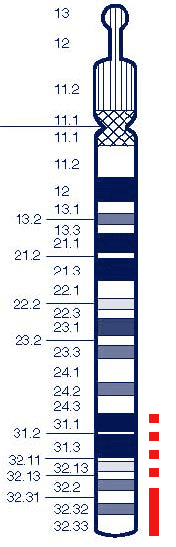
Each chromosome has a short arm (at the top of the diagram on the next page), which is called the p from pet, and a long arm (at the bottom) by the French word for small. We believe that the short (p) arm of chromosome 14 is very small and can replicate without apparent harm. The extra genetic material from the long arm is expected to yield more results because this part contains important genetic information.
Chromosomes are not visible to the naked eye, but when magnified under a microscope, they are visible after staining with a dye that shows a characteristic band pattern. The diagram on page 3 shows the bands of chromosome 14, numbered outward from the centromere (the hollow part of the chromosome that divides into two arms). There are few numbers close to the centromere, such as q11. The region close to the centromere is called proximal. Many chromosomes, such as q32, are located near the tips of the chromosomes and are called distal because they are far from the centromere.
Karyotype
Genetics experts can tell you more about which chromosomes are missing. It is almost certain that chromosomes are broken and a karyotype is given, which is a shortened code that shows the recombined bands. Bands contain many genes, and depending on the technique used to test for duplication of your child’s chromosomes, a karyotype can also show whether a particular gene is duplicated. However, you should seek a thorough explanation from a genetics expert.
Your child’s karyotype may look like someone else’s, it may look unique or from medical literature, or it may look exactly the same. However, even people with the same karyotype may have chromosome breaks at different locations within the same band. This is one important reason why people with apparently similar karyotypes do not all have the same problems and characteristics. Individual differences are very noticeable and it is very important not to directly compare your child to others. After all, each of us is unique. However, some characteristics and health problems are similar in people with 14q duplication . This brochure contains similar information.
Does it matter which parent the extra portion of 14q comes from?
The extra portion of chromosome 14 comes from either the mother or father, and the effects may differ depending on which parent it comes from. This is due to a phenomenon known as imprinting, in which certain parts of chromosomes have different effects depending on their parent of origin. The effect of imprinting on 14q duplication is that an affected infant or child is given a single dose of the gene from one parent and two doses of the gene from the other parent. It is known that certain genes on chromosome 14 are imprinted, and people who have two 14q arms from their mothers are significantly different from people who have two 14q arms from their fathers. (see the Unique leaflet for uniparental disomy 14). An association has been found between specific features of the
14q duplication and specific regions of chromosome arms. Some evidence comes from six consanguineous relatives from one family who appear to be completely normal, with the exception of one child with overlapping small bands within 14q31 and moderate developmental delay. Met. This duplication was maternally inherited, suggesting that this small maternally inherited duplication of 14q31 may not be deleterious in general. In another family with different small duplications within band 14q31 , the most severely affected children inherited the duplication from their mothers, so in this family the effect was milder if the duplicated material was inherited from the father. (see page 5 for families with duplication without obvious effects).
As we will see, information about the effects of imprinting is still evolving (Palmer 2006; Sutton 2002; MignonRavix 2001; Georgiades 1998; Robin 1997).
Sources and references
Some of the information contained in this brochure is taken from published medical literature. In many cases, detailed molecular analysis of the chromosomes has not been performed, and 14q duplications are often combined with deletions or duplications of another chromosome , but this is currently the best information available.
PubMed allows you to search for abstracts and original articles on the Internet by first named author and publication date.
You can also obtain abstracts and articles from Unique.
This brochure also utilizes Unique’s database. At the time this leaflet was written, Unique had 44 members with chromosome 14q duplications , 24 of whom had pure 14q duplications . Eighteen families completed detailed questionnaires in 2006.
Complete duplication (trisomy) of 14q
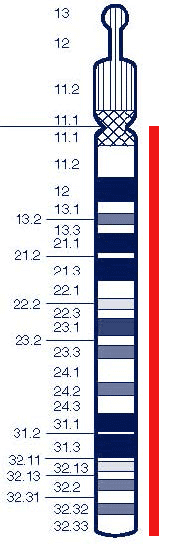
It is also possible to conceive a baby with the full length arm of chromosome 14. This is most common when one parent has a Robertsonian translocation, which causes the long arm of chromosome 14 to fuse with the long arm of the other chromosome. Chromosome 13 has the highest frequency, followed by chromosome 21, chromosome 15, chromosome 22, and chromosome 14. However, pregnancy loss is common, and neonates with a complete 14q overdose generally do not survive to birth. The overwhelming majority of infants who survive have cells with a normal number of chromosomes and cells with an extra 14q. This is known as mosaic trisomy 14. The problems faced by children with mosaic trisomy 14 tend to be more severe than those faced by children with partial duplication, including delayed growth and development, abnormal facial features (wide, upturned nose, abnormally formed or placed noses, etc.) . These include large ears, small mandibles, and short necks), congenital heart defects, and, in boys, small genital anomalies.
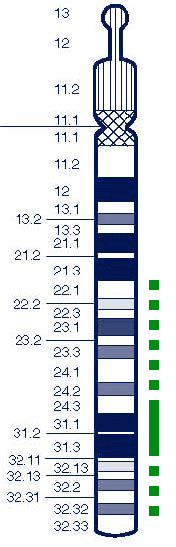
This leaflet discusses duplication of part of chromosome 14q . The large duplication between 14q22 and 14q32 is thought to involve the ends of the long arms, as well as duplications extending proximally and distally to 14q13 .
Large overlap between 14q22 and 14q32
Eight cases have been reported in the medical literature, including one case in which multiple family members were affected, and a unique member with smaller duplications within bands 14q31 and q32 . Furthermore, at least 12 consanguineous relatives in three families have been reported with a small duplication of band 14q31 showing a large duplication from 14q24.3 to 14q31, with no apparent impact on development (Palmer 2006; Mignon- Ravix 2001 ; Robin 1997; North 1995; Rivera 1992; Gilgenkrantz 1990/2; Mikelsaar 1987; Sobel 1984; Nikolis 1983; Orye 1983; Unique).
Duplication of bands 14q22~24~14q32
Reports of individuals with a duplicate segment of 14q22~24~14q32 include a 29-year-old and his Nehu (Rivera 1992; Gilgenkrantz 1990/2; Mikelsaar 1987; Sobel 1984; Nikolis 1983; Orye 1983). Characteristics were generally less specific but included low birth weight (2.25 kg/4 lb 15 oz to 2.9 kg/6 lb 6 oz), short stature in childhood, developmental delay, language delay, and learning difficulties.
The reported health problems are so serious that two infants have developed heart problems, one with a ventricular septal defect (VSD) and one with a hole between the lower chambers of the heart. . Specific treatment for VSDs is determined on an individual basis as small holes may close spontaneously, whereas large VSDs usually require surgical repair. One child was seriously ill and had a posterior urethral valve (a blockage in the valve that drains urine from the bladder), kidney failure, and underdeveloped lungs. Vision, as well as hearing, can be affected, including temporary impairment due to glue ears. A further child (with 14q22q24.3 duplication) had nasal obstruction requiring corrective surgery (villous atresia), immunodeficiency, large VSD, and genital abnormalities (North 1995). In this group, two neonates died, one at 4 months and one at 10 months.
Some cases had slightly abnormal features on the hands, including a single palmar crease and short or tapered fingers. Two infants with 14q24q32 duplications had a similar pattern in which the thumb long and middle fingers overlapped with adjacent digits. Two children were born with talus varus (clubfoot), which caused the foot to point downward and inward, usually requiring surgical correction. Focusing on individuals with slightly smaller overlap
between 14q23.3 and 14q32.3 , the effects were generally milder and the degree of general developmental delay was milder. Regarding mobility, from the available information rolling over is achieved at about 6-7 months, sitting for about 9-15 months, independent mobility around the first birthday and walking in the second half of the second year. achieved.
However, all were nonambulatory, and the child with the 14q22q24.3 duplication was still not walking or talking at 4.5 years.
Small overlap within band 14q31~14q32
Two major clinical questions have emerged from the unique and limited information available. One child with a duplication within band 14q32 developed absence seizures, which were controlled with antiepileptic drugs. Another child has short eyelids and can no longer close his eyes. This condition is seen in other patients with 14q duplications and requires surgical correction, after which vision appears to develop normally (see Haley, pages 12-13).
Development was also affected, with moderate retardation of mobility, hypotonia (hypotonia) and walking achieved in the second or third year. Although there is no specific information regarding fine motor skills, one child had significant difficulty holding a pencil for writing after 7 years. The age of reading suggests that these children began reading between 6 and 8 years of age, while they were talking between 3 and 4 years of age. About 4 years ago, I succeeded in keeping it clean and dry every day (unique).
Families with overlap and no clear effect
In one family, six members had the same duplication of band 14q31 inherited from the mother , but in five cases there was no obvious effect on development or growth. In the sixth family member, duplication probably played no role in his developmental delay (Mignon-Ravix 2001). In another family, four members had a small duplication of part of band 14q31 . Although the individual family members had a variety of problems, including developmental delays and cataracts, the one family member with the duplication was clinically and developmentally normal, so the small duplication found was probably not the cause of the problem. There was no (Palmer 2006). In one father, the father was paired with a daughter with a duplication of 14q24.3q31 , with the father unaffected and the daughter mildly affected (Robin 1997).
A possible explanation for some of these findings is that duplication may have different effects depending on the parent of origin (see which parent the extra fragment of 14q comes from). page 3
Large duplication of the ends of the long arms from 14q13 to 14q24.3
Eleven babies and pregnancies have been reported in the medical literature, including three members who have a pure duplication of the long arm of chromosome 14q , starting between 14q13 and 14q24.3. This corresponds to duplication of between one-third and two-thirds of the long arm of the chromosome . Often duplications occur with deletions or duplications from another chromosome , but here we have individuals with pure duplications, or duplications involving the short arms of chromosomes 13, 14, 15, 21, and 22. Only individuals with this combination have been described, and these are not expected to influence outcome. This is followed by individual stories of unique members with 14q duplications and combinations of deletions or greater duplications.
In general, a unique experience is that its membership is better than its depiction in the medical literature (Ohtake 1994; Duckett 1990; Nakamura 1990; Gilgenkrantz 1990/1; McCorquodale 1985; Kaiser 1984; Sklower 1984; Atkin 1983 ; Cohen 1983; Georgmaneanu 1981; Pfeiffer 1978; Fryns 1977; Trunca 1977; Weinstein 1977; Unique).
Of her eight pregnancies, two ended in premature birth. Birth weights of term infants ranged from 1.83 kg (4 lb 1 oz) to 3.8 kg (8 lb 6 oz), which was higher than the average weight for newborns. Many babies grew into short children. Unfortunately, many babies have major medical problems, especially overcoming heart defects and large blood vessel abnormalities, which occurred in 7 out of 14 babies.
Medical literature describes various symptoms, including a large herniation of the diaphragm separating the contents of the abdomen from the chest, small kidneys with multiple cysts, absence of the corpus callosum (a wide band of nerve fibers connecting the two hemispheres of the brain), and convulsions. We are seeing serious problems. In addition, four newborns, including two girls, had abnormalities in the genital area, and at least one had severe visual defects. Unfortunately, two newborns died within the first few months of life. Two unique members with a 14q duplication and another chromosome deletion or duplication also died as a result of respiratory infections in both cases.
Slight malformations of both limbs and certain facial features are common in infants and children with chromosomal abnormalities, but are of primary concern to families when they affect the child’s functioning. Infants with large 14q duplications had duplications of the fifth toe, fingers, and toes, and one infant had calcaneus valgus (clubfoot), a deformity in the position of the foot that points outward and downward. be. Among the abnormal facial features observed are a prominent forehead, prominent nose, small chin, lower jaw, abnormal ears, prominent upper lip, high forehead, and fontanelles (soft spots on the top of the head) that close The eyes were slow and turned downward, and the eyes were widely set apart, possibly showing sparse hair growth.
The roof of the mouth may become abnormally high or narrow. An extremely rare finding in one infant is abnormal development of the lower eyelid, making it difficult or impossible to close the eye and requiring surgical correction. This defect was also observed in two unique members with small terminal duplications of 14q (see Gilgenkrantz 1990, Haley, pp. 12-3).
Most newborns have either hypotonia (lower muscle tone, which makes them feel weaker) or a combination of hypotonia and hypertonia, which means they have increased muscle tone. Ta. Developmentally delayed, the baby required significant support to achieve developmental milestones such as sitting.
Information on the late development of children with large distal 14q duplications is limited, but one young male with a large duplication from 14q21 and a small deletion from the end of the short arm of chromosome 3 (3p25 breakpoint) was written at the age of 27. In his case, he passed puberty normally, but 10 years later than expected.
Andrew
Andrew has a deletion from the end of the long arm of chromosome 1 , with a breakpoint at 1q44, and a duplication of about one-third of the long arm of chromosome 14 , with a breakpoint at 14q24.3.
At birth, Andrew was slightly underweight at 2.4 kg (5 pounds, 5 ounces) and had abnormally low muscle tone. She was breastfed, but lactation was slow and her growth rate followed the lowest curve on the growth curve for the first 9 months of life, when she entered solid food and began to catch up. At the age of 10 he weighed 27 kg and just over 4 stone although he was rather shorter than his school friends.
Andrew is generally healthy and catches the normal range of colds and coughs that affect young children. Tear duct infections are treated with antibiotics. he was wearing glasses. When he was five years old he underwent surgery to have his testicles removed. His testicles had not descended into his scrotum. He was born with small teeth in the front of his mouth. These eventually fell off, and the adult teeth replaced them in normal time.


Although Andrew’s general development is delayed, he has made significant progress since age 9. At age 10, he still required personal care, but was able to eat with a fork and drink from a sealed cup with an integrated straw. He also mastered the computer mouse and TV remote control.
Andrew’s primary means of walking is walking. He likes to hold an adult’s hand when walking on uneven surfaces or long distances, and his family uses a stroller outdoors. Andrew can climb stairs with an adult, but cannot get up from the floor by himself.
Andrew’s feet are small and have little arch.
To stimulate sensation in Andrew’s legs and other muscles, his family used an innovative treatment known as dotting therapy. Although this is a specific physical therapy that has not been objectively evaluated over a long period of time, it is known that intensively applied physical therapy is likely to have short-term benefits. Reports of attempts to explore treatments are available from Unique. Unique, on the other hand, does not endorse any particular innovative treatment, but rather encourages families to seek individual treatment for their child from a physical therapist or physiotherapist. Andrew is sociable, proud of himself, and has self-esteem. If people invade his personal space, he can make a strong point of attack, but his family praises good behavior and makes others understand that Andrew is uncomfortable being too close. Manage this by letting
Andrew’s first language was sign and he had a vocabulary of over 400 words by the age of five. By 10 o’clock, the signing had been decided among those who were not yet used to the event. After the age of 9, he began to vocalize more and more, sometimes using long and complex sentences, but his speech was still immature and many consonants were not yet fully developed. Andrew’s understanding is much greater than his ability to express himself, but he can ask, for example, “Can I leave the table now?” Andrew is an enthusiastic and successful learner. He uses a computer with an IntelliKeys keyboard, learns well and is encouraged when tasks fail. He remembers his name and face. As long as he deals with handover guidance, Andrew can write and learn mathematics. No one person alone can tell you that one and one are equal. But with this guidance, you can add, subtract, and multiply to tables and division 12 times.
He has a high literacy rate. At the age of eight, his spelled age was considerably older than his actual age. At 10 o’clock he could read children’s books, newspaper headlines, TV guides, children’s prayers, and the Bible. His family says it’s difficult to judge when he reads alone, but by age 11, when he was reading in bed, he was telling them to go away.


Small duplication at the end of the long arm starting at 14q31 or 14q32
Three adults, the oldest 29 years old, and three children have been described in the medical literature with pure duplication of the long arm end starting at band 14q31. Among unique members, one child has a pure duplication from 14q32 , as well as other chromosomal deletions or duplications (2, 4, 5, 6, 9, 15, 18 or 22) on 14q. Many children also have a distal duplication of (Palmer 2006; Sutton 2002; Mignon-Ravix 2001; Magnani 1993; Masada 1989; Carr 1986; Trunca 1977; Weinstein 1977; Unique).
Reports in the medical literature indicate that growth retardation is common before and after birth and can be very pronounced, with one patient, a 24-year-old, having the average height of an 8-year-old. Although growth retardation was inconsistent, three neonates had normal birth weight, and a 5-year-old neonate with a duplication from 14q32.1 had normal weight and length.
The degree of developmental delay is also expected. Significant delays in reaching the developmental milestones of rolling over and sitting were observed, and at least two had strongly contracted joints; one adult was unable to walk. Little information is available about learning ability, although one child could speak a few words by the age of 3, and one adult was functioning at the level of an 11-year-old child, but another of adults were unable to speak.
Most patients were generally healthy, but one child had complex malformations of the heart and great vessels, a defect in the neural tube exposing the spinal cord (lumbosacral myelomeningocele), and two lesions in the brain. Cerebral malformations were found with partial loss of the corpus callosum, a broad band of nerve fibers that normally connect the hemispheres. A 19-year-old woman with a mosaic duplication of 14q32.1 , i.e., a woman with cells in her body with the duplication and an otherwise normal chromosomal composition, had frequent respiratory tract infections and seizure disorders. .
In general, Unique’s experience is that its members are better than depictions in the medical literature suggest.
Becky

Becky lost the tip of the long arm of chromosome 15 at a break point at 15q26.3, and the end of chromosome 14 was duplicated from 14q31.3. The main impact of her chromosomal abnormality was on her development, and she also had health problems. By the time she was 16 years old, Becky was a young lady and although she had a cheerful disposition and happy demeanor, her developmental problems were significant.
She said Becky was born a month early, weighing 2.69 kg (5 lbs 15 oz) and she did not cry during her birth although she was breathing. Her fontanel (soft spot) was very large and she attracted the attention of her doctors. She had a small hole made in her heart and eventually recovered on her own, but was otherwise healthy.
Becky later developed health problems, including seizures between the ages of 3 and 11 and frequent ear infections in infancy, but by the age of 16 she was generally healthy and well into her adolescence. The period progressed normally.
Eating was a constant challenge as a baby and child, but she made steady progress. She was unable to breastfeed, so she was fed with a nasogastric tube for four months, and then she was artificially fed. By the time she was 2 years old, she could stir and drink her food and could take 3 small pieces of her cake. And she was able to take a loaded spoon into her mouth. By 5 o’clock she was able to eat with a spoon and drink from the feeder cup. By 10 o’clock, once she cut her food into bite-sized pieces, she could eat on her own. As a teenager, she had a good appetite, sometimes filling her mouth and choking, but she was growing and gaining moderate weight. However, Becky was small at 144 cm (4’9) at the age of 16. Becky’s mobility is quite delayed and in her early childhood many of her joints are flaccid and in some cases unstable due to her low underlying muscle tone while , excessive tension and muscle contracture became a problem that increased over time.
She was walking on her stomach by age 2 and she was walking by age 5, but her balance gradually improved over the next few years. She required regular physical therapy, passive stretching, splinting, and gaiters to combat her joint contractures, but by 10 years she was a confident swimmer. Yes, and by 10 years it was running in an unstable condition.
Becky’s fine motor skills also lagged behind, but by five years she was able to point and manipulate objects, draw a straight line in eight, take off her coat in ten, and hang herself on a peg. He lowered it and tried to use a large knife.
Becky is sociable and popular, and although her dialogue is very limited, it is well conveyed through her first-hand experiences and some signatures, gestures, and dynamite communication aids. Her understanding is greater than her ability to express herself. Becky’s level of communication reflects her learning ability. Her concentration problems improved during her elementary school years, but were still noticeable. As a teenager, she could use a basic keyboard. Becky has been working with a behavioral therapist to address her challenging behavior and successfully respond to those close to her and consistent boundaries.
She has the most wonderful smile and a friendly, sociable personality and enjoys being all over the place, albeit very tired.
Davis

Davis has a deletion from the end of the long arm of chromosome 18 , with a breakpoint at 18q23, and the end of the long arm of chromosome 14 has been duplicated with a breakpoint at 14q31.3. His remarkable facial features, including his sparse eyebrows, low-set ears, far-set eyes, and wide smile, were discovered six weeks ago after he was born. Davis faced considerable challenges as a newborn. He had difficulty feeding, had a gastrostomy tube placed at 5 weeks of age, had a tracheostomy at 6 weeks (removed at age 3), had difficulty breathing, and had chronic respiratory syncytial virus (RSV). (causing respiratory infections). A week later, Davis underwent an MRI and CT scan of his head and brain, which showed complete agenesis of the corpus callosum, the bundle of nerve fibers that connects the two hemispheres of the brain. Davis had a good birth weight for a premature baby, but he has slipped down the growth curve and is now the size of a 4-year-old instead of a 12-year-old. From age 3 to age 10, Davis took growth hormone shots, but these were ineffective and were discontinued. Davis’ chronic RSV resulted in multiple hospitalizations from his birth until age 7. On average, patients spent about two and a half months per year recovering from RSV and complications.
At age 12, Davis is now 4 1/2 years old without hospitalization and appears to be outgrowing RSV. He won an award last year for his perfect school attendance rate. Davis is very nearsighted and has mild hearing loss that does not require hearing aids. His ear canal was very narrow and he had surgery to correct this in his right ear when he was four years old. Although Davis has global developmental delay, he is not classified as having mental retardation or intellectual disability. The consensus of his medical team is that Davis is cognitively capable, but he doesn’t know how he knows what he knows. Davis did not start walking until he was 6 years old, and by age 12 he was still using a walker and wheelchair. He can sit in a chair, use stairs (with help), and even run using a walker. Davis is a very social and happy child who loves playing with his “typically developing peers”, especially during his lessons. Although Davis’ speech is limited, he is believed to understand 90% of what is said. Since he was two and a half years old, he can compose complete sentences on the computer, the best educational tool he has worked with. Communication with his colleagues has increased with the help of his assistive technology device, Springboard. Davis is currently in his fourth year (being taught in a regular education classroom). Ms. Davis, a third-grader, grew up with her classmates, who have been together since kindergarten. Davis has benefited from a one-on-one instructional assistant. Assistants help facilitate teaching in regular education classrooms.
Boo

Boo has an additional chromosome consisting of the short arm of chromosome 9, a small piece of the long arm, and the end of chromosome 14, which consists of 14q32.1. The patient was born after an uneventful pregnancy, good weight and good condition. He breastfed for 6 weeks without any problems other than cracked gums. Boo grew steadily and by the age of 13 he was average height for his age. Boo developed asthma in infancy, which was treated with a surgically healed umbilical hernia (a bulge that covers the inside of the abdomen, and sometimes part of the abdomen wraps around the navel), an inguinal hernia, tubes, and pneumonia. However, the company’s growth exceeded that of the previous health concerns. Boo is also short-sighted and has convergent squid (seeing inside the eye), which was corrected with laser surgery. He developed hydrocephalus (excess fluid in the brain) as an infant and was treated with a shunt. Regarding his appearance, Boo has some unusual features. Some of their toes overlap, they have abnormal ears, and the back of their heads is flat. When he was a baby, a soft spot (fontanelle) had grown on his head.
Boo’s development has been supported by language, vocational, physical therapy and special education. He had low muscle tone and mobility was somewhat delayed. By 9 months he could sit, walk and climb stairs at 3 years, and run at 7 years. By 13:00, he was handling a knife and had a pencil, but although he could write his first name and letters of the alphabet, he could not apply enough pressure.
At school he enjoyed using the entire keyboard. He has a good memory, especially for directions and rap music, and enjoys playing the drums with both hands. Although his speech progressed well, he still had difficulty with word order and tension, and improved his stunmer using a fluid device (SpeechEasy).
At the age of 13, Boo was experiencing adolescence. In his family, Boo is full of affection and loves adult attention. He can sometimes be too kind to strangers.
Emel
Emer loses the end of the long arm of chromosome 22 from 22q13.31 (Phelan-McDermid syndrome) , and the end of chromosome 14 is duplicated from 14q32.1 . The main problems are eating, sleeping, anxiety, toileting, and communication.
Other than common childhood illnesses, she was generally healthy until age 7, with tests showing that her lungs, kidneys, and brain were healthy. She was 15 months old at birth, although her weight was good and despite her early latching problems, she was breastfed with a nipple shield. She had problems with solid foods and when she was sick she was prone to inhaling food and getting respiratory infections. Until she was 6 years old, Emel’s food was pure, and she took in calories and nutritional supplements to help her gain weight. At 7 years old, she still has difficulty chewing.

Emel had low muscle tone, but with physical therapy input, he walked for three years with the help of a walker and climbed five flights of stairs. She receives input from speech therapy and uses a variety of communication methods including signs, symbols, gestures, photographs, body language, facial expressions, pointing, communication books, references, and spoken word. Her longest sentence to date is “Mommy, help me.” At school at the age of seven, Emer began looking at pictures, drawing lines, and using touchscreens that allowed him to write. As long as she repeats the lessons regularly, she has a good memory. Emer is potty trained and she suffers from bladder urgency/frequency. She doesn’t sleep well and suffers from anxiety.
Haley
Hayley lost the short arm end of chromosome 5 at 5p15.31 , and the end of chromosome 14 was duplicated at 14q32.11. She has the same karyotype as Esme (see pages 13-4), but the effects are different. Deletion 5p typically causes a genetic syndrome known as Cri du Chat (named after the cat-like cry of babies with the disease), where the tip of chromosome 5p is missing. may not cause the typical features of this syndrome. Hayley has an unusual condition seen in other children with A14Q duplication , where she is unable to close her eyes because her lower eyelids are underdeveloped . After repeated skin grafts and four surgeries, the blockage in her eye has improved, but she is susceptible to infections and requires artificial tears to prevent it from drying out too much.
By the age of nine, Hayley was generally in very good health, but had numerous hospitalizations to deal with various conditions. Nissen to improve the operation of duodenal webs (membranes of the intestinal tract causing obstruction), ectopic anus (anus in front of its normal position), cleft palate, etc., and the valve between the food passage and the stomach These include fundectomy, insertion of a gastric tube and button to allow direct feeding into the stomach, removal of tonsils, and numerous chest infections. The patient continued to have constipation and asthma, which were controlled with medication.
Haley had very small feet and at 9, his feet were that of a 7-8 year old baby. Developmentally, she was able to move her legs to stand and walk with her support. The three crooked fingers of her hand were splinted like a baby, making it easier for her to hold things. She communicates with her gestures and sounds and understands more than she can say. At school she is a determined learner and is supported with a SEN statement. She is generally happy and friendly, and particularly enjoys rough and tumble games. The rougher the better.


Without her, I would lose myself. Thanks to her, I can’t stop laughing every day. What else do I need?
Esme
In Esme, the end of the short arm of chromosome 5 is missing from 5p15.31 , and the end of chromosome 14 is duplicated from 14q32.11. She has the same karyotype as Hayleigh (above) but is affected differently. Esme is missing the region at 5p13.31, which is associated with the typical cat-like meow and plaintive voice of Cri du Chat syndrome . Although she doesn’t have any major health issues, she has been hospitalized for eating disorders, pneumonia, urinary tract infections and reflux, bronchitis, and gastroenteritis. When she was 2 weeks old, she had only one seizure, which was probably a febrile seizure.
Esmie, who had stopped growing in the womb, was induced at 38 weeks and was very small at birth. As a newborn, we were concerned about her inability to hold onto her feet and her weakened muscles. By feeding her high-calorie milk, her weight increased by 50% after 7 months, but her body length and head circumference were on a 3% curve. Esme experienced a twilight episode after her feeding and was diagnosed with regurgitation and aspiration, where her breast milk flows back up the food passageway and is inhaled into the lungs. The reflux was controlled with concentrate feed and medication to keep the feed in the stomach. Recently, she started having hypoglycemic attacks (low blood sugar levels). These symptoms often occur after a mild illness and are currently under investigation.
Very small limbs, facial features include sparse eyebrows, high forehead, wide flat bridge of nose, large chin, very pronounced groove between nose and upper lip, rather small lower jaw, and slightly prominent upper lip. And so on.
At 14 months it is too early to tell how she will develop, but she is very sociable and responsive and remembers people well. Although her Esme can sit independently and she has shown that she can roll over, she chooses not to roll over.
Since she was born she has had physical and occupational therapy and from 8 months on conduction education.


She seems so loving and happy that it’s contagious.
Roller
Laura lost the end of the long arm of chromosome 4 from 4p16.3 , and the end of chromosome 14 was duplicated from 14q32.2.
Deletion of terminal band 4p16.3 causes Wolf-Hirschhorn syndrome , but Laura does not have the classic features of this well-known chromosomal abnormality. Although she is young and has mild developmental delays, by the age of eight she learned to walk and ride a bicycle. She first used the word twice and spoke in short sentences eight times. She attended mainstream school and learned to read and write to a level that was probably typical for a three-year-old child. She loved playing and being social with other children. She was perfectly healthy. Laura exhibited a slightly abnormal facial appearance and an eye movement disorder known as Duane syndrome on the left side, but did not require treatment.
Aaron

Aron loses the end of the short arm of chromosome 18 from 18p11.31 , and duplicates the end of chromosome 14 from 14q32.3 . Although she was born after a normal pregnancy, she had an unexpectedly low birth weight and one or two malformations, including a small head and undescended testicles.
After suction and oxygenation at birth, Aron coped, but had difficulty feeding and swallowing. Allophen was found to have no major birth defects, but died frequently from viral infections, and six had recurrent chest infections and were taking anti-asthma medication. He has also experienced 2 to 3 febrile convulsions, but has not been diagnosed with epilepsy. Aron also has stomach problems and severe constipation.
Aron needs a lot of help maintaining his mobility as he is not yet able to sit or walk, but he can roll from side to side. At 6 he can’t grasp or grasp yet, but he can swim with toys and operate switch devices from his head. His muscle tone is abnormally high and he takes the muscle relaxant Baclofen. Aaron communicates vocally and with his eyes, and in special school he has proven to be a regular learner with a good memory.
He seems very happy and likes being with his family, so he contributes a lot to our life.
How did the duplication occur?
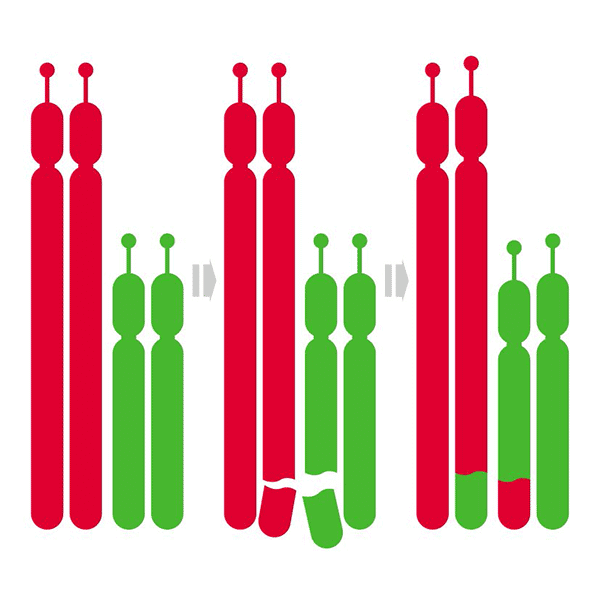
The 14q duplication is the result of a chromosomal rearrangement in one parent. This is usually a balanced translocation, in which material is exchanged between the chromosomes, but no material is lost or gained, so the parents usually have no health or developmental problems. Sometimes we find that one parent has the same overlap with the child.
Other 14q duplications occur when both parents have normal chromosomes . The term geneticists use for this is de novo (dn).
The new 14q duplication is caused by changes that normally occur when the parents’ sperm or egg cells are formed. We know that chromosomes must be broken and reattached when eggs and sperm cells are formed, but this only sometimes causes problems.
Disconnection and reattachment is part of a natural process and as a parent you cannot change or control it. Children from all parts of the world and from all types of backgrounds have 14q overlap . No environmental, dietary, or lifestyle factors are known to cause these There was no indication that the parents had caused the duplication before or during pregnancy, and nothing could have been done to prevent it.
Will it happen again?
The possibility of another pregnancy with a 14q duplication depends on the chromosomes of the parents. If both parents have normal chromosomes, the 14q duplication is very unlikely to occur again.
If blood tests show that either parent has a chromosomal change involving 14q, other pregnancies with chromosomal changes are more likely. Once you know your family’s chromosomal changes, future pregnancies can be tested to see if your child’s chromosomes are affected.
Discussing chromosomal changes with other family members can help other family members get blood tests to find out if they have chromosomal changes.
A genetics expert can give your family more guidance.
Support and Information
Rare Chromosomal Anomalies Support Group,
G1, The Stables, Station Road West, Oxted, Surrey RH8 9EE, United KingdomPhone
/Fax:+44(0)1883 723356
info@rarechromo.org I www.rarechromo.org
Join unique for family links, information and support.
Unique is a charity that no government funding and relies solely on donations and grants.
It is made up of funding and grants. If you are able, please receive through our website. www.rarechromo.org Thank you for your cooperation.
This information guide is not a substitute for personal medical advice. Families should consult a medically qualified clinician regarding all matters related to genetic diagnosis, management, and health. Information about genetic changes is a very fast-moving field, and while the information in this guide is believed to be the best available at the time of publication, some facts may later change. there is. Unique does its best to stay abreast of changing information and review published guides as necessary. This guide was compiled by Unique and co-authored by Dr. Edmond Lemire, Head of Medical Genetics, Royal University Hospital, Saskatoon, Canada, and Marj, Professor of Reproductive Genetics, University of Warwick, UK. -Reviewed by Professor Halten BSc PhD MD FRCPath.
Copyright (Unique 2007 edition)
Rare Chromosome Abnormalities Support Group Charity Number 1110661
Registered in England and Wales Company Number 5460413
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。

