

Article Summary
This article provides an overview of capillary malformation syndrome, MEF2C-related disorders, and Usher syndrome type 2, all of which are known as hereditary rare diseases. It covers the symptoms caused by each condition, necessary treatments and management, their genetic background, and the support systems required for patients and their families.
Genes likely to be strongly involved in disorders at this locus

| S/N | Gene Name | Japanese Disease Name | Associated disease name |
| 1 | RASA1 | Capillary Malformation–Arteriovenous Malformation Syndrome | Capillary Malformation-Arteriovenous Malformation Syndrome |
| 2 | MEF2C | MEF2C-Related Disorder | MEF2C-Related Disorder |
| 3 | ADGRV1 | Usher Syndrome Type 2 | Usher Syndrome Type 2 |
[1_RASA1] Capillary Malformation–Arteriovenous Malformation Syndrome (CM-AVM)

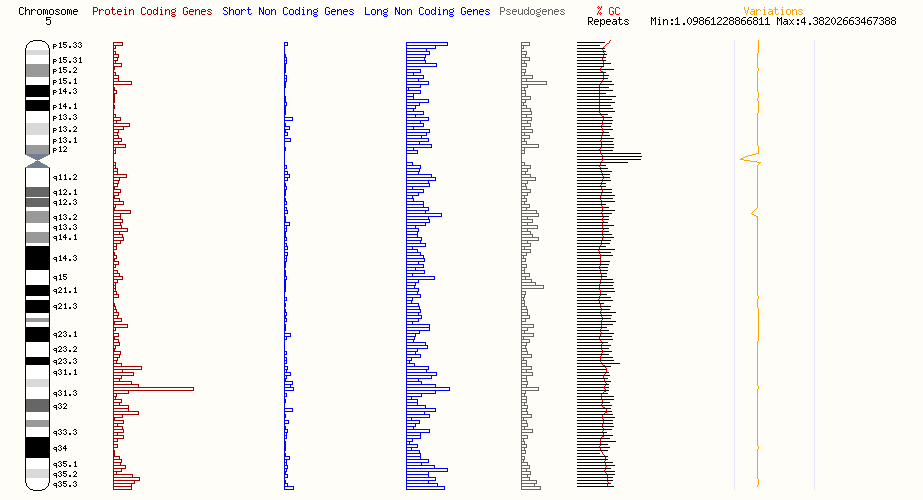
Capillary Malformation–Arteriovenous Malformation Syndrome (CM-AVM) is a hereditary disorder that causes vascular abnormalities. The main cause is mutations in the RASA1 gene, which is located in the 5q14.3 region of chromosome 5. This gene plays an important role in controlling the Ras/MAPK pathway, which regulates cell growth, differentiation, and proliferation. Mutations in the gene impair normal blood vessel formation, leading to the characteristic symptoms of this disease.The main symptoms of this disorder are capillary malformations (CMs) that appear on the face and limbs. These lesions are small, about 1–2 cm in diameter, pink to reddish-brown in color, and round or oval in shape. Some lesions may show a white halo (a pale surrounding area). In addition, high-flow vascular abnormalities such as arteriovenous malformations (AVMs) and arteriovenous fistulas (AVFs) can occur in the skin, muscles, bones, spine, and brain. These vascular abnormalities can cause life-threatening complications such as bleeding, heart failure, and neurological symptoms. Especially AVMs or AVFs in the brain may manifest in early childhood, requiring early diagnosis and management.

Diagnosis is based on clinical features. Specifically, when capillary malformations or arteriovenous malformations are confirmed, and when pathogenic variants in RASA1 or EPHB4 are identified by genetic testing, a definitive diagnosis is made. Family history is important, as risk assessment and early diagnosis are critical. Genetically, CM-AVM is autosomal dominant, with a 50% chance of inheritance in the children of an affected patient. For RASA1, about 70% of mutations are inherited and 30% are de novo. For EPHB4, 80% are inherited and 20% are de novo.
Treatment aims to relieve symptoms and reduce the risk of complications. If capillary malformations are of cosmetic concern, dermatological evaluation is recommended. For arteriovenous malformations or fistulas, careful assessment of the suitability of embolization or surgery is necessary. If there is cardiac involvement, a cardiologist should be consulted, and if there are leg-length discrepancies or hemihyperplasia, orthopedic consultation is recommended.

Some patients with this disorder also show symptoms of Parkes Weber Syndrome, characterized by red vascular skin lesions, micro-arteriovenous fistulas, and overgrowth of soft tissue and bone. These symptoms usually appear in childhood. Lymphatic abnormalities have also been reported, and in cases of lymphedema, compression stockings are effective.
Regular follow-up is essential, especially with imaging studies for AVMs and AVFs that may progress. For vascular abnormalities in the brain or spine, early detection is crucial, so screening of these areas is recommended. When there is a family history, genetic testing of at-risk relatives can help establish preventive management.
The prevalence of CM-AVM varies by region. In Northern Europe it is estimated at 1/100,000, but recent studies report incidence rates of 1/20,000 for RASA1 mutations and 1/12,000 for EPHB4 mutations. Although the prevalence is relatively low, the diversity and severity of symptoms make early diagnosis and comprehensive medical management essential.

At the molecular level, RASA1 controls the Ras/MAPK pathway and regulates vascular development. Loss of this function causes abnormal blood vessel development. On the other hand, EPHB4 is specifically expressed in venous endothelial cells and regulates arteriovenous differentiation. Loss of this protein can cause abnormal vascular development.
CM-AVM syndrome is clinically and genetically very heterogeneous, and individualized management is required. Early diagnosis and appropriate treatment interventions by specialists aim to improve the quality of life of affected patients.
[2_MEF2C] MEF2C-Related Disorder

MEF2C-related disorder is a rare genetic disease characterized mainly by neurodevelopmental delay. This disorder severely affects language development and motor skills. Specifically, most patients have profoundly limited speech ability and many cannot walk independently. Hypotonia is prominent, interfering with movement and posture control. In addition, patients may show distinctive facial features, seizures, visual or cardiac abnormalities, and autism-like behaviors (reduced social interaction and repetitive hand movements).
With respect to speech, most patients can only use a few words and cannot form sentences. Regarding walking, about half of patients cannot walk independently, though walking may be possible with assistance or devices.

Diagnosis is made by molecular genetic testing, specifically by identifying heterozygous pathogenic variants in the MEF2C gene. MEF2C encodes an essential transcription factor that regulates cell development and function, and mutations cause a wide range of symptoms centered on the nervous system.
Currently, there is no curative treatment, and therapy is symptomatic. Supportive care includes developmental and educational programs, walking assistance by orthopedists and physical therapists, nutritional management, and treatment of reflux or constipation. Anti-epileptic drugs are used for seizures, and cardiologists and ophthalmologists manage heart and vision problems. In cases of recurrent respiratory infections or otitis media, antibiotics or ear tube insertion may be recommended. Psychological and social support for patients and families is also important.

MEF2C-related disorder follows an autosomal dominant inheritance pattern, but most cases reported to date are due to de novo mutations. In rare cases, mutations may be inherited from an affected parent, or from a parent with mosaicism. If inherited, the chance of passing on the pathogenic variant is 50%.
Characteristic symptoms include developmental delay, intellectual disability, hypotonia, feeding and gastrointestinal issues, distinctive facial features (broad forehead, prominent philtrum, everted upper lip, large ears), seizures, autism-like behaviors, sleep disturbances, congenital heart defects (such as ventricular septal defect, patent ductus arteriosus), and visual abnormalities (such as strabismus and refractive errors). Brain MRI may show hypoplasia of the corpus callosum, thinning of the white matter, ventricular enlargement, and delayed myelination.
Early intervention programs are recommended, including physical, occupational, and speech therapy, as well as feeding support. Alternative and augmentative communication (AAC) methods may be considered when speech is limited, ranging from picture cards to high-tech speech-generating devices. For autism-related behaviors, applied behavior analysis (ABA) therapy may be effective.
The MEF2C gene plays a critical role in neurodevelopment and embryogenesis, and loss of function is the main cause of this disorder. While future research may lead to effective therapies, current care focuses on symptom management and improving quality of life.
[3_ADGRV1] Usher Syndrome Type 2

Usher Syndrome Type 2 (USH2) is an inherited disorder, mainly caused by mutations in the ADGRV1 gene located in the 5q14.3 region. The main features are congenital hearing loss and progressive retinitis pigmentosa (RP). In some patients, vestibular dysfunction may also occur.
The clinical features of USH2 include bilateral sensorineural hearing loss, mild-to-moderate at low frequencies and severe-to-profound at high frequencies. This hearing loss is usually present from birth, and audiograms typically show a “sloping” pattern. Some individuals may perceive progression over time, though the degree varies among patients.

RP is a bilateral progressive retinal disease, beginning with night blindness and constricted visual fields (“tunnel vision”) and later causing central vision loss. The progression and severity of vision loss differ among individuals. RP first affects rod cells (responsible for night vision) and later cone cells (responsible for daylight vision). Vestibular function may be normal, mildly impaired, or subclinically affected.Diagnosis is based on hearing and vision evaluations, including audiometry, electroretinography (ERG), visual field testing, and optical coherence tomography (OCT). Definitive diagnosis is confirmed by identifying biallelic pathogenic variants in ADGRV1, USH2A, or WHRN.

Treatment for hearing loss includes early fitting of hearing aids and speech training. If hearing aids are insufficient or hearing loss is severe, cochlear implantation may be considered. For RP, standard supportive management is used, with some studies exploring nutritional supplements such as vitamin A (though high doses may be harmful, especially in pregnancy).
Regular follow-up is essential: annual hearing assessments with hearing aids or implants, and annual ophthalmologic evaluations (particularly after age 20) to detect RP progression or complications such as cataracts or cystoid macular edema.
Daily life adaptations are needed to prevent accidents due to tunnel vision and night blindness. Driving may become unsafe, especially at night, and should be avoided.

USH2 is inherited in an autosomal recessive manner. If both parents are carriers, the child has a 25% risk of being affected. Genetic counseling is important for families, and prenatal or preimplantation diagnosis may be considered when risk is high.
The prevalence of USH2 is estimated at a few per 10,000 individuals. It accounts for 3–6% of childhood deafness and about 50% of combined hearing and vision impairment. Because RP symptoms often appear after adolescence, diagnosis is often delayed.

At the molecular level, the proteins encoded by ADGRV1, USH2A, and WHRN form the “Usher interactome”, a network maintaining sensory neuron health in the inner ear and retina. Disruption of this network results in the symptoms of USH2.
USH2 is clinically and genetically very heterogeneous. Comprehensive evaluation and management tailored to each patient are required. Improving understanding of this disease is key to enhancing quality of life for patients and families. Early diagnosis and appropriate therapy are essential to maximize potential.
References
- Koenekoop R, Arriaga M, Trzupek KM, et al. Usher Syndrome Type II. 1999 Dec 10 [Updated 2023 Mar 23]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1341/
- Cooley Coleman J, Skinner SA. MEF2C-Related Disorder. 2024 Dec 12. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK610216/
- Bayrak-Toydemir P, Stevenson DA. Capillary Malformation-Arteriovenous Malformation Syndrome. 2011 Feb 22 [Updated 2019 Sep 12]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK52764/
- Perez, G., Barber, G. P., Benet-Pages, A., Casper, J., Clawson, H., Diekhans, M., Fischer, C., Gonzalez, J. N., Hinrichs, A. S., Lee, C. M., Nassar, L. R., Raney, B. J., Speir, M. L., van Baren, M. J., Vaske, C. J., Haussler, D., Kent, W. J., & Haeussler, M. (2024). The UCSC Genome Browser database: 2025 update. Nucleic Acids Research, gkae974. https://doi.org/10.1093/nar/gkae974
- Harrison, P. W., Amode, M. R., Austine-Orimoloye, O., Azov, A. G., Barba, M., Barnes, I., Becker, A., Bennett, R., Berry, A., Bhai, J., Bhurji, S. K., Boddu, S., Branco Lins, P. R., Brooks, L., Budhanuru Ramaraju, S., Campbell, L. I., Carbajo Martinez, M., Charkhchi, M., Chougule, K., … Yates, A. D. (2024). Ensembl 2024. Nucleic Acids Research, 52(D1), D891–D899. https://doi.org/10.1093/nar/gkad1049
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







