

Article Summary
Williams Syndrome (WS) is a rare genetic disorder that affects neurodevelopment, physical features, and the cardiovascular and endocrine systems. This article provides up-to-date information on the symptoms, diagnosis, and treatment of WS. It highlights the importance of early diagnosis and comprehensive care, and offers guidance on how to support patients and their families in achieving a better quality of life.
Overview

Williams Syndrome (WS) is a rare genetic disorder that affects multiple body systems, most notably neurodevelopment. It is characterized by a combination of distinct physical features, developmental challenges, and various medical complications.
People with WS often have characteristic facial features, such as a broad forehead, a narrow temple area, puffiness around the eyes, star-like or lace-patterned irises, a short upturned nose with a rounded tip, a long philtrum (the area between the nose and upper lip), a wide mouth, full lips, and mild underdevelopment of the lower jaw (micrognathia).
Developmental and intellectual delays are also common in WS. Intellectual disability is typically mild, though individuals often have a unique cognitive profile. Language skills tend to be a relative strength, whereas spatial reasoning is often an area of difficulty. Many individuals also display a distinct personality, often characterized by extreme friendliness (overfriendliness) and difficulty regulating emotions.
Cardiovascular involvement is another hallmark of WS. The most common cardiac issue is supravalvular aortic stenosis (narrowing above the aortic valve). Other cardiovascular problems can include peripheral pulmonary artery stenosis and hypertension. In addition, connective tissue abnormalities—such as joint hyperflexibility and overly elastic skin—are common and can contribute to delayed motor development. Low muscle tone (hypotonia) and excessive joint flexibility often delay the acquisition of motor milestones.
Endocrine problems are also frequently seen in WS. These may include early-onset puberty (precocious puberty), elevated calcium levels in the blood (hypercalcemia) or urine (hypercalciuria), and hypothyroidism. Many individuals experience growth delays, often resulting in shorter adult stature compared to average. Feeding difficulties during infancy and slow weight gain are also common.
WS affects approximately 1 in 7,500 individuals, with males and females equally affected. Because the impact of this syndrome spans multiple systems, comprehensive multidisciplinary care tailored to each patient’s needs is essential.

Causes and Diagnosis
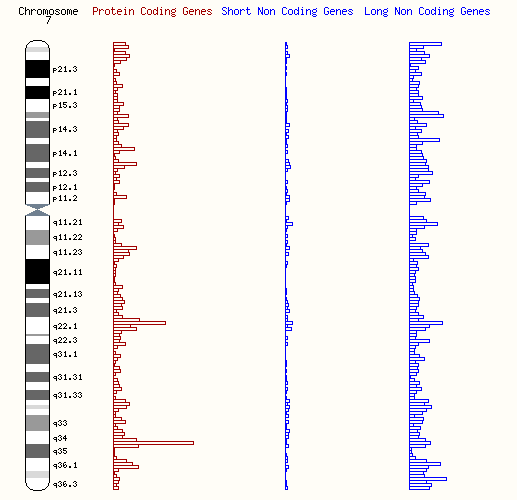
Williams Syndrome (WS), also known as Williams-Beuren Syndrome, is caused by the deletion of a specific region on chromosome 7 (7q11.23). This deletion typically spans 1.5–1.8 megabases (Mb) and involves approximately 25–28 genes. In most cases, this deletion occurs spontaneously and is not inherited from the parents.
The deleted region is flanked by areas of low copy repeats (LCRs), which are repetitive sequences. During the process of meiosis (the formation of eggs or sperm), these repetitive sequences may misalign due to their high similarity, resulting in unequal crossing-over and causing the deletion responsible for WS. Among the genes affected, the elastin gene (ELN) is the most studied. Loss of one copy of the ELN gene (haploinsufficiency) is directly linked to arterial stenosis, one of the most common clinical features of WS. While other genes within the deleted region are also implicated in the syndrome, many of their specific roles remain unclear, though some genotype-phenotype correlations have been established.
Because this deletion affects multiple genes, it explains the wide range of physical characteristics, developmental challenges, and medical issues seen in WS. Therefore, diagnosis and management often require a comprehensive, multidisciplinary approach.Diagnosis of WS typically begins with recognition of the syndrome’s characteristic physical and developmental features (phenotype) and is confirmed through genetic testing. Common diagnostic tools include fluorescence in situ hybridization (FISH) and chromosomal microarray analysis, both of which detect deletions in the 7q11.23 region. With advances in DNA sequencing technology, non-invasive prenatal testing (NIPT) has become a reliable and safe option for detecting WS during pregnancy, posing no risk to the mother or fetus.

Genetic counseling is an important part of managing WS and should be offered to affected families. Most cases are de novo (spontaneous), meaning the deletion is not inherited from the parents. As a result, the recurrence risk in future pregnancies is very low (less than 1%). However, if an individual with WS has children, there is a 50% chance of passing the deletion to their offspring. In rare cases, the presence of certain inversion polymorphisms in the chromosomal region may slightly increase the risk of having a child with WS.
Symptoms and Management
Williams Syndrome (WS) is a complex neurodevelopmental disorder caused by the deletion of the 7q11.23 region on chromosome 7. In about 95% of cases, the deletion is around 1.5 Mb, but in approximately 1 in 20 cases, a larger 1.84 Mb deletion is present. WS affects multiple systems, causing characteristic facial features, developmental delays, cognitive challenges, and a range of medical problems.
All individuals with WS have distinctive facial features (craniofacial dysmorphism). In early childhood, these include epicanthal folds (skin folds at the inner corner of the eyes), full cheeks, a flat facial profile, and small, widely spaced teeth. As they grow, their face often becomes more elongated, and their neck may appear longer. Developmental milestones such as walking and language acquisition are typically delayed, and approximately 75% of individuals have intellectual disabilities. Cognitively, language and short-term memory are relative strengths, but significant deficits in visuospatial processing are common. Personality traits often include marked sociability and a deep interest in music, though hypersensitivity to sound (due to absent auditory reflexes) is also frequently observed. Emotional regulation difficulties are common, and about 50% of individuals require support for anxiety disorders or attention-deficit/hyperactivity disorder (ADHD).

Cardiovascular problems are present in about 80% of individuals with WS. The most common issue is supravalvular aortic stenosis, affecting around 70% of patients. Other cardiovascular problems include hypertension (50%) and degenerative changes of the aortic or mitral valves. Endocrine abnormalities are also common, with 15–45% of patients experiencing hypercalcemia, glucose intolerance, or type 2 diabetes; 15–30% experiencing subclinical hypothyroidism; and 50% experiencing reduced bone mineral density (osteopenia or osteoporosis). Additional issues can include axial hypotonia (weakness in trunk muscles), increased limb tone (hypertonia), brisk reflexes, cerebellar ataxia, tremors, growth delays (about 75% of the normal rate), hyperflexible joints in early childhood, joint contractures with age, gait abnormalities, spinal issues (lordosis, kyphosis, scoliosis), eye, ear, and dental anomalies, sleep disturbances, feeding difficulties, gastrointestinal problems, bladder diverticula, urinary tract malformations, urinary tract infections, and nocturnal enuresis.Management of WS requires a lifelong, multidisciplinary approach. Cardiac evaluations during the first year of life and close monitoring of calcium levels during the first two years are especially important. Surgical procedures carry higher cardiovascular risks, making careful pre- and postoperative planning essential. Early intervention programs—including physical, occupational, and speech therapy—are critical for addressing developmental delays. Providing information and access to support groups for patients, families, and caregivers can significantly improve quality of life.
Although the genetic basis of WS is well understood, the molecular mechanisms underlying its diverse symptoms remain incompletely explained. Recent genome-wide studies have identified abnormal gene pathways potentially associated with WS, providing new directions for research and the development of targeted therapies.
Prognosis
The average life expectancy of individuals with WS has not been formally established, but cardiovascular complications remain the leading cause of death. Vascular narrowing often progresses during the first five years of life but may improve spontaneously in cases like peripheral pulmonary artery stenosis. Most individuals require lifelong medical care and daily support at home or in work environments.
Recent studies have shown favorable long-term outcomes for WS patients undergoing cardiovascular surgery. For those who survive the first five years after congenital heart defect surgery, the survival rate over the next 30 years exceeds 90%. Advances in medical care and accessibility have steadily improved the prognosis for children with WS. Early and accurate diagnosis, particularly through non-invasive prenatal testing, allows families to prepare adequately and seek timely medical interventions.

reference
- Morris CA. Williams Syndrome. 1999 Apr 9 [Updated 2023 Apr 13]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1249/
- Li, H. H., Roy, M., Kuscuoglu, U., Spencer, C. M., Halm, B., Harrison, K. C., Bayle, J. H., Splendore, A., Ding, F., Meltzer, L. A., Wright, E., Paylor, R., Deisseroth, K., & Francke, U. (2009). Induced chromosome deletions cause hypersociability and other features of Williams–Beuren syndrome in mice. EMBO Molecular Medicine, 1(1), 50–65. https://doi.org/10.1002/emmm.200900003
- Schubert, C. (2009). The genomic basis of the Williams – Beuren syndrome. Cellular and Molecular Life Sciences, 66(7), 1178–1197. https://doi.org/10.1007/s00018-008-8401-y
- De Cegli, R., Iacobacci, S., Fedele, A., Ballabio, A., & Di Bernardo, D. (2019). A transcriptomic study of Williams-Beuren syndrome associated genes in mouse embryonic stem cells. Scientific Data, 6(1), 262. https://doi.org/10.1038/s41597-019-0281-5
- Zinyandu, T., Montero, A. J., Thomas, A. S., Sassis, L., Kefala-Karli, P., Knight, J., & Kochilas, L. K. (2023). Thirty-Year Survival After Cardiac Surgery in Children With Williams-Beuren Syndrome (from the Pediatric Cardiac Care Consortium Study). The American journal of cardiology, 187, 48–53. https://doi.org/10.1016/j.amjcard.2022.10.037
- Orphanet. (Last updated March 2021). Williams syndrome. Reviewed by Dr Pernille GREGERSEN, Dr Mette HANDRUP, Dr Anne LEEGAARD. Retrieved from https://www.orpha.net/en/disease/detail/904?name=Williams-Beuren%20syndrome&mode=name
- Perez, G., Barber, G. P., Benet-Pages, A., Casper, J., Clawson, H., Diekhans, M., Fischer, C., Gonzalez, J. N., Hinrichs, A. S., Lee, C. M., Nassar, L. R., Raney, B. J., Speir, M. L., van Baren, M. J., Vaske, C. J., Haussler, D., Kent, W. J., & Haeussler, M. (2024). The UCSC Genome Browser database: 2025 update. Nucleic Acids Research, gkae974. https://doi.org/10.1093/nar/gkae974
- Harrison, P. W., Amode, M. R., Austine-Orimoloye, O., Azov, A. G., Barba, M., Barnes, I., Becker, A., Bennett, R., Berry, A., Bhai, J., Bhurji, S. K., Boddu, S., Branco Lins, P. R., Brooks, L., Budhanuru Ramaraju, S., Campbell, L. I., Carbajo Martinez, M., Charkhchi, M., Chougule, K., … Yates, A. D. (2024). Ensembl 2024. Nucleic Acids Research, 52(D1), D891–D899. https://doi.org/10.1093/nar/gkad1049
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







