
Salwati SHUIB PhD, Nenny Noorina SAAID MMedSc, Zubaidah ZAKARIA* MBBS, DCP, Juriza ISMAIL **
MBBS, MMed and Zarina ABDUL LATIFF** MMed, MSc
Department of Pathology, National University of Malaysia Medical Center, * Hematology Unit, Medical Research Institute Cancer Research Center, ** Department of Pediatrics, National University Malaysia Medical Center, Kuala Lumpur.
Summary
Potocki‐Lupski syndrome (PTLS) , also known as duplication 17p11.2 syndrome , trisomy 17p11.2 or dup(17)(p11.2p11.2) syndrome, is a developmental disorder and rare contiguous genetic syndrome that affects 20,000 live births. 1 person will be affected. The main characteristics of such patients are autism spectrum disorder, learning disabilities, developmental delay, attention deficit disorder, infantile hypotonia and cardiovascular abnormalities. Previous studies using microarrays have identified variations in the size and extent of the duplicated region of chromosome 17p11.2 . However, there are a small number of genes that are considered candidates for PTLS , including RAI1, SREBF1, DRG2, LLGL1, SHMT1 and ZFP179 . In this report, we investigated the case of a 3-year-old girl with developmental delay.
Her chromosome analysis showed a normal karyotype (46,XX). Analysis using array CGH (4X44 K, Agilent USA) identified a novel duplication of approximately 4.2 Mb in chromosome 17p11.2. The results were confirmed by fluorescence in situ hybridization (FISH) using a probe of the critical PTLS region.
This report demonstrates the importance of microarray and FISH in the diagnosis of PTLS .
Keywords : Potocki-Lupski syndrome , duplication 17p11.2 , microarray, developmental delay, fluorescence in situ hybridization
Introduction
Chromosome 17p11.2 duplication syndrome (OMIM #610883) , also known as Potocki Lupski syndrome (PTLS) , was first described by Brown et al . Subsequently, with the advent of high-resolution methods such as microarrays, more patients were reported. 2 , 3 Molecular analysis of the PTLS region showed that it is the same region deleted in Smith Magenis syndrome.
(OMIM #182290) consists of unique mating fragments with apparent fragment sizes. This region was also described to be preferentially paternal in origin and to arise by the non-allelic homologous recombination (NAHR) mechanism . The majority of patients had a common 3.7 Mb duplication within the 17p11.2 range, and the remainder had non-recurrent duplications ranging from 1.3 to 15.2 Mb. A critical PTLS region was identified as 1.3 Mb long, including the retinoic acid inducible 1 (RAI1) gene and 17 other genes .
The common phenotype of patients with PTLS is hypotonia, poor feeding, failure to thrive, developmental delay in infancy, language impairment, hyperactivity in infancy, intellectual disability, autism and behavioral disorders in older children. , and cardiovascular problems. 5 , 6 Variations in the size of the overlap region can explain the wide diversity and severity in clinical features of PTLS patients. In this study, the authors identified microduplication 17p11.2 in children with global developmental delay . The size of the overlap is estimated to be 4.2 Mb, which overlaps the common and critical region of PTLS .
Case Report
The patient was a 3-year-old girl, the second child of an unrelated marriage. She presented to UKMMC’s Child Development Center (CDC) with problems of hyperactivity, developmental delay, central hypotonia and poor weight gain. She weighed 2890g at birth and was delivered full term by caesarean section. Her mother is 39 years old and was diagnosed with gestational diabetes during her pregnancy. During her early infancy, the patient was active, but she had slow suckling during breastfeeding. Forty-eight hours after her birth, the patient was admitted to the neonatal intensive care unit due to respiratory depression secondary to hypoglycemia. The patient was referred to the physical therapy department and she started walking at the age of two. She could run, climb stairs and walk step by step, but she could not go down stairs. She could speak 11 words meaningfully and follow simple instructions. She was unable to feed herself and she had enuresis, enuresis, every day. Her hearing and ocular evaluation were normal.
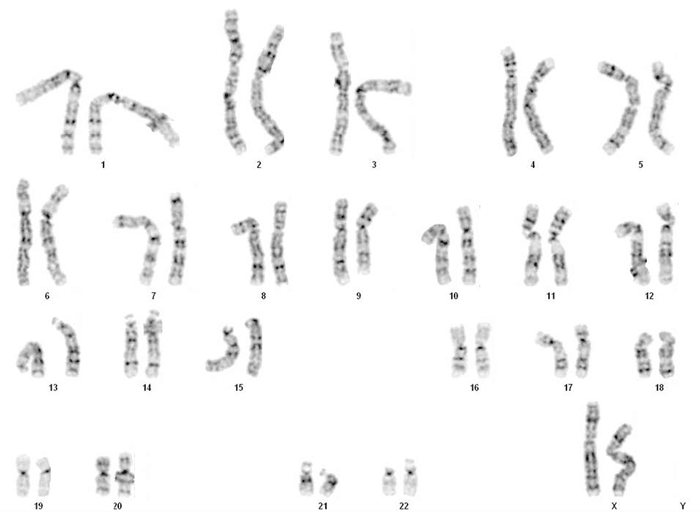
Informed consent was obtained from the parents for this case report. The study protocol and informed consent were approved by the University Kebangsaan Malaysia Research Committee Board. Genetic Findings Blood lymphocyte cultures were prepared from patient blood samples according to standard protocols. Giemsaband chromosomes were analyzed from 20 metaphases showing a normal female karyotype at a haploid (bph) resolution of 550 bands ( Fig. 1 ).
Genomic DNA was extracted from patient blood samples using the DNeasy Blood & Tissue kit following the manufacturer’s recommended procedure (Qiagen, Germany). Regular commercially available female gDNA (Agilents Technologies, USA) was used as a standard sample. DNA quality and quantity was assessed using electrophoresis in 1.0% agarose gels and a NanoDrop UVVIS spectrophotometer (Nanodrop Tech). Array CGH was performed on Agilent Human Genome 4x44K oligonucleotide array slides according to Agilent’s Direct Method of Oligo Array CGH workflow (Agilent Technologies, USA), respectively. As a result of microarray analysis, an approximately 4.2 Mb duplication was detected on chromosome 17p11.2 ( Figure 2 ).
The start and end points of duplication were estimated to be 16,782,546 and 21,050,337 kb, respectively. This region contains 122 RefSeq genes, including genes from the important PTLS region.

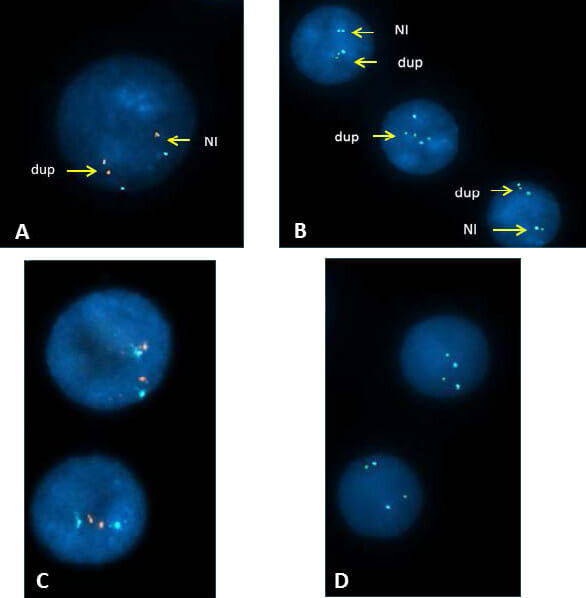
Considering previous reports and the contents of the genomic variant database (http://dgv.tcag.ca/gb2/gbrowse/dgv2_hg19/), this duplication is considered to be a characteristic of the Potocki-Lupski syndrome duplication , and the dose-sensitive RAI1 To confirm the microarray results, we tested the specific probes Agilent SureFISH 17p11.2 GLL1-SHMT1 (spectral red), Agilent SureFISH 17p11.2 RAI1 (spectral green) and the control Agilent SureFISH 17 CEP BL (spectral aqua). ) was used to perform FISH. Hybridization results on 150 nuclei analyzed showed evidence of duplication of the RAI1 and SHMT1 loci , confirming the microarray findings.
Both parents had normal karyotypes (data not shown) and normal FISH signal patterns: 2 red, 2 green, and 2 aqua ( Fig. 3 ).
Consideration
Array CGH identifies, at high resolution (≤1 Mb), copy number variations (amplifications or deletions) and single copy gains/losses across entire chromosomes and the genome, providing accurate information related to the physical and genetic map of the human genome. location information. 7 This technology has become more cost-effective and affordable, and many laboratories, including in middle-income countries, have begun to utilize it as a first-line diagnostic test in patients with learning disabilities. 8 However, it is important to note that this technique does not allow for the identification of balanced translocations, and therefore investigations of patients with learning disabilities and congenital anomalies must always include conventional karyotyping. .
Evidence from a study conducted by the International Standard Cell Genome Array (ISCA) Consortium shows that first-step cytogenetic diagnosis of patients with developmental delay/intellectual disability, autism spectrum disorders, and multiple birth defects Chromosomal microarray should be applied as a test. This is mainly due to its higher sensitivity compared to traditional G-band analysis. 9 Furthermore, a large systematic review of 13,926 subjects with learning disabilities (mental retardation) and congenital anomalies supports the routine use of array CGH in the study of such patients with normal karyotyping. There is evidence to support this. However, the study also suggests that the results should be interpreted with caution. This is because the technique identifies as many false positives as it does the causative variant. 8
Using microarray and FISH validation, the authors identified an approximately 4.2 Mb duplication of 17p11.2 in their patients associated with PTLS . The overlap region identified in our patient overlaps with the 3.4 Mb common region and 1.3 Mb critical region of PTLS (Figure 2). In addition to the common phenotype of PTLS , our patient was also noted to have neonatal hypoglycemia. It is well known that women with diabetes (gestational diabetes, pregestational diabetes) are at increased risk of having children with hypoglycemia. Therefore, neonatal hypoglycemia in our patient was most likely due to maternal gestational diabetes rather than a redundant effect . FISH analysis and karyotyping performed on the parents’ blood samples showed normal results, indicating that PTLS in this patient occurred as a de novo event.
Although the majority of reported PTLS cases are de novo, there have been two reports (in three families) of hereditary PTLS to date. 10 , 11 Recently, Lee et al. 12 found a shortest 0.25 Mb (17,575,978-17,824,623) duplication of 17p11.2 in a boy with a subtle PTLS phenotype. The duplicated region lies within the critical PTLS region and includes only four genes: RAI1, SMCR5, SREBF1 and TOM1L2. Consistent with previous reports, they suggested RAI1 as an important dose-sensitive gene involved in the main clinical features of the PTLS phenotype, and SREBF1 as another potential candidate gene. However, it remains unclear whether PTLS is caused by duplication of only the RAI1 or SREBF1 loci . Studies in mouse models have also provided evidence that Rai1 is an important and dose-sensitive gene involved in the PTLS phenotype . 13 , 14
In conclusion, our findings demonstrate the importance of array CGH and interphase FISH in identifying and confirming the 17p11.2 duplication (PTLS), which would have been missed when routine Giemsa band (G band) chromosomes alone were analyzed. showed that. 550 banding per haploid resolution (bph) can detect chromosomal aberrations, including deletions or additions of 5 Mb or more, but for smaller aberrations (<5 Mb) higher band resolution or alternative Therefore, more specialized techniques such as FISH, array CGH, sequencing or NGS would be the best approach to resolve this chromosomal rearrangement.
Acknowledgment
We would like to thank all the patients and parents who participated in this clinical trial. We would also like to thank the staff of the Cytogenetics Unit, Department of Pathology, UKMMC for their technical attitude and support. This research was supported by Universiti Kebangzan Malaysia for UKM-GUP-2011-320 and FF-2013-329.
The authors declare that they have no conflict of interest.
References
- Brown A, Phelan MC, Patil S, Crawford E, Rogers RC, Schwartz C. Two patients with 17p11.2 duplication: the reciprocal of the Smith-Magenis syndrome deletion? Am J Med Genet. 1996; 63: 373-7.
- Potocki L, Chen KS, Park SS, et al. Molecular mechanisms of duplication and reciprocal homologous recombination of the 17p11.2-Smith-Magenis microdeletion. Nat Genet 2000; 24: 84-7.
- Potocki L, Bi W, Treadwell-Deering D, et al. Characterization of Potocki-Lupski syndrome (dup(17)(p11.2p11.2)) and the dose-sensitive critical interval that can convey the autism phenotype. depiction. Am J Hum Genet. 2007; 80: 633-49.
- Zhang F, Potocki L, Sampson JB, et al. Identification of rare recurrent Potocki-Lupski syndrome-associated duplications and distribution of rearrangement types and mechanisms in PTLS. Am J Hum Genet. 2010; 86: 462-70.
- Soler-Alfonso C, Motil KJ, Turk CL, et al. PotockiLupski syndrome: a microduplication syndrome associated with oropharyngeal disorders and failure to thrive. J Pediatr. 2011; 158: 655-9.
- Jefferies JL, Pignatelli RH, Martinez HR, et al. Cardiovascular findings in duplication 17p11.2 syndrome. Genet Med. 2012; 14: 90-4.
- Cheung SW, Shaw CA, Yu W, et al. Development and validation of a CGH microarray for clinical cytogenetic diagnosis. Genet Med. 2005; 7: 422– 32.
- Sagoo GS, Butterworth AS, Sanderson S, ShawSmith C, Higgins JP, Burton H. Array CGH in patients with learning disabilities (mental retardation) and birth defects: an updated systematic review and meta-analysis of 19 studies and 13,926 cases. Genet Med. 2009; 11:139-46.
- Miller DT, Adam MP, Aradhya S, et al. Consensus statement: Chromosomal microarrays are first-line clinical diagnostic tests for individuals with developmental disorders or congenital abnormalities. Am J Hum Genet. 2010; 86: 749–64.
- Yusupov R, Roberts AE, Lacro RV, Sandstrom M, Ligon AH. Potocki-Lupski syndrome: hereditary duplication with left heart hypoplasia (17) (p11.2p11.2). Am J Med Genet A. 2011; 155A: 367-71.
- Magoulas PL, Liu P, Gelowani V, et al. Expanding the hereditary dup(17)(p11.2p11.2): Potocki-Lupski syndrome phenotype. Am J Med Genet A. 2014; 164A: 500-4.
- Lee CG, Park SJ, Yim SY, Sohn YB. Clinical and cytogenetic features of Potocki-Lupski syndrome with the shortest 0.25 Mb microduplication in 17p11.2 containing RAI1. Brain Department 2013; 35: 681-5.
- Walz K, Paylor R, Yan J, Bi W, Lupski JR. Duplication of Rai1 causes physical and behavioral phenotypes in a mouse model of dup(17) (p11.2p11.2). J Clin Invest. 2006; 116: 3035-41.
- Carmona-Mora P, Walz K. Retinoic Acid Induced 1, RAI1: a dose-sensitive gene associated with neurobehavioral changes including autistic behavior. Cargenomics 2010; 11: 607-17.
Contact: Dr. Salwati Shuib, Cytogenetic Unit, Department of Pathology, Jalan Yaacob Latif, Bandar Tun Razak, Universiti Kebangsaan Malaysia Medical Center (UKMMC), Cheras 56000 Kuala Lumpur, Malaysia. Phone number: 603-91459511, Fax number: 603-91459485 Email: salwati@ppukm.ukm.edu.my
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







