
この記事のまとめ
This article unpacks the latest evidence on Nablus Mask-Like Facial Syndrome, from its genetic basis to its distinctive mask-like facial features and associated systemic symptoms. It also explains how the condition is diagnosed, highlights best practices for multidisciplinary care, and explores emerging research that may shape future understanding and treatment of this rare disorder.
Overview
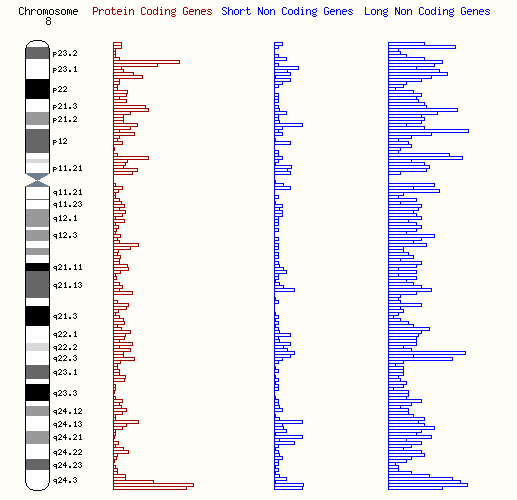
Nablus Mask-Like Facial Syndrome (NMLFS) is a rare congenital genetic disorder caused by a microdeletion on the long arm of chromosome 8, specifically within the 8q21.3–8q22.1 region. The condition was first described in 2000 by geneticist Ahmad Teebi, who identified the syndrome in a boy from Nablus, Palestine. Since that first report, only around 26 cases have been documented worldwide as of 2024, making it one of the rarest known chromosomal microdeletion syndromes. Over the years, further clinical observations have confirmed that NMLFS represents a distinct genetic condition characterized by unique craniofacial morphology, developmental delays, and a variable range of systemic abnormalities.
Because of its rarity, much of what is currently known about NMLFS comes from individual case reports and small cohort studies. These sources have helped shape the understanding of the syndrome but also highlight the wide variability in its presentation, which complicates diagnosis and management.
Alternate Names

NMLFS is also known in medical literature by several alternate names, including 8q22.1 Microdeletion Syndrome, Monosomy 8q22.1, and, in cases where clinical overlap exists, Blepharo-Naso-Facial Syndrome. These alternative terms reflect attempts to describe either the genetic basis or the phenotypic characteristics of the syndrome prior to the establishment of its current name.
Distinctive Clinical Features
Facial Characteristics
The name “mask-like facial syndrome” refers to the most consistent and recognizable aspect of the condition: a distinctive, expressionless facial appearance. This mask-like effect is the result of a specific combination of craniofacial anomalies. Many individuals have narrow eye openings, or blepharophimosis, coupled with skin that appears taut and shiny, particularly over the nasal bridge. Eyebrows tend to be sparse and arched, while the nasal bridge itself is broad and flat, often with a rounded tip. An upswept frontal hairline is common, giving the hair a characteristic upright growth pattern at the midline.
The midface and jaw structures are also affected. The philtrum, the vertical groove between the upper lip and nose, is often elongated and smooth. The lower lip frequently appears everted, and the lower jaw, or mandible, is underdeveloped, a condition known as micrognathia. Some patients also exhibit hypoplasia of the upper jaw, known as maxillary hypoplasia. Bilateral cheek dimples and dysmorphic ears with poorly formed rims are additional features that contribute to the distinctive facial presentation.
Interestingly, many individuals with NMLFS are described as having a bright and sociable temperament, a behavioral contrast to the relative immobility of the facial musculature that gives the syndrome its name.
Clinical Variability
Despite these characteristic features, the syndrome exhibits significant variability. Not all patients with the 8q22.1 microdeletion present with the full spectrum of craniofacial characteristics. Some exhibit atypical or subtle facial differences, while others express a phenotype more consistent with the classic description. This variability highlights the concept of variable expressivity, where the same genetic change can manifest differently in each individual.

Systemic and Developmental Characteristics
Growth and Neurodevelopment
Most individuals with NMLFS show some degree of developmental delay. Motor and speech development are commonly affected, with delays becoming evident in early childhood. Intellectual ability often ranges from mild to moderate intellectual disability, and microcephaly, or a head size smaller than the average for age and sex, is frequently reported.
Musculoskeletal and Joint Features
The musculoskeletal system is commonly involved. Hypotonia, or low muscle tone, is a frequent finding in infants and young children, often contributing to delays in motor milestones. Over time, joint contractures may develop, restricting mobility, and camptodactyly, a condition where one or more fingers remain permanently bent, is sometimes observed. Some children also present with a sandal gap deformity, characterized by an unusually wide spacing between the first and second toes.
Genital Abnormalities
In males, genital anomalies are relatively common. Cryptorchidism, or undescended testes, and hypoplastic scrotum have been reported in multiple cases, requiring surgical assessment or intervention.
Oral and ENT Differences
Craniofacial differences often extend to the oral cavity and upper airways. Many patients have a protruding upper jaw or a high-arched palate. Some present with a submucous cleft palate or, less frequently, a visible cleft lip. Dental anomalies are also a common finding, ranging from congenital absence of certain teeth to enamel hypoplasia and malocclusions such as open bite. Thickening of the jaw ridge and macroglossia, or an enlarged tongue, may further complicate oral function. Hearing impairment, typically sensorineural in nature, has been documented, as has laryngomalacia, a softening of the laryngeal structures that can lead to noisy breathing or airway difficulties in infancy.
Other Organ System Involvement
NMLFS can affect multiple organ systems beyond the face and musculoskeletal structures. Hernias, particularly inguinal or abdominal wall hernias, have been observed. Cardiovascular malformations such as patent ductus arteriosus occur in a subset of patients. Gastrointestinal anomalies, including malrotation of the intestines, have also been noted.
More recent reports describe progressive myopathy, or muscle disease, developing in adulthood in some patients. This finding suggests that the clinical presentation of NMLFS may evolve over time, underscoring the importance of long-term follow-up and monitoring.
Genetic Mechanism and Diagnosis
Chromosomal Basis
The underlying cause of NMLFS is a microdeletion on chromosome 8, within the 8q21.3–8q22.1 region. The size of the deletion varies, ranging from approximately 1.6 megabases (Mb) to 8.9 Mb. Comparative genomic analyses of reported cases have allowed researchers to narrow the critical region most closely associated with the syndrome to an approximately 2.8 Mb segment, located between 93.5 Mb and 96.3 Mb on the GRCh37/hg19 reference genome. This region contains several genes of interest, including TMEM67, CCNE2, GDF6, ESRP1, and RAD54B. While these genes are strong candidates for explaining the syndrome’s craniofacial and systemic manifestations, direct causal links remain under investigation, and research is ongoing to clarify their precise roles.
Inheritance Patterns
Most cases of NMLFS are the result of de novo deletions, meaning the chromosomal change arises spontaneously in the affected individual and is not inherited from either parent. However, rare cases of familial inheritance have been documented, suggesting an autosomal dominant inheritance pattern with incomplete penetrance and variable expressivity. This means that a person carrying the deletion may not always display the full clinical picture, or any symptoms at all, complicating genetic counseling.
Diagnostic Methods
Diagnosis of NMLFS requires molecular genetic testing, particularly when the facial or systemic findings suggest a chromosomal microdeletion. High-resolution chromosomal techniques such as array comparative genomic hybridization (array-CGH) and chromosomal microarray analysis (CMA) are the most commonly used tools for detecting deletions in the relevant region. Fluorescence in situ hybridization (FISH) is useful for localizing specific deletions and can also detect mosaicism in complex cases. Whole exome sequencing (WES) is increasingly applied when the clinical presentation is atypical, as it can identify both sequence-level mutations and copy number variations.
Non-invasive prenatal testing (NIPT) has gained attention for its potential to identify microdeletion syndromes, including NMLFS, in utero. By analyzing cell-free fetal DNA circulating in maternal blood, NIPT offers a safer and less invasive alternative to traditional diagnostic methods such as amniocentesis, though confirmatory testing remains necessary for definitive diagnosis.
Management and Support
Effective management of NMLFS requires a multidisciplinary approach tailored to the individual’s needs. Pediatric neurologists, clinical geneticists, pediatric surgeons, dentists, ear-nose-throat (ENT) specialists, and psychologists often work together to provide coordinated care. Early developmental support, including physical therapy, speech therapy, and behavioral interventions, can significantly improve outcomes for children with motor or communication delays. Surgical interventions may be necessary to address complications such as cryptorchidism, joint contractures, or cleft palate.
Regular monitoring is also important. Growth parameters, hearing function, and cardiac health should be evaluated periodically to identify and address emerging issues. Psychosocial support is an integral component of care, particularly for older children and adolescents, to help them navigate social and emotional challenges associated with their appearance and communication difficulties.
Prognosis
The long-term outlook for individuals with NMLFS is highly variable and depends on the severity of the symptoms. Children with milder presentations may achieve functional independence with appropriate medical and developmental support, while those with more complex needs often require ongoing, lifelong care. Recent evidence of adult-onset myopathy highlights the importance of continued medical follow-up beyond childhood.
With early intervention and consistent multidisciplinary management, many children with NMLFS can achieve an improved quality of life despite the unique challenges posed by this rare syndrome.
Research Outlook
Because NMLFS is so rare, further research is critical to expand understanding of its genetic and clinical spectrum. Detailed genomic studies, particularly in patients with smaller deletions of less than 2 Mb, may help identify which genes drive specific clinical features. Longitudinal studies are also essential to better understand how the condition evolves with age and to guide evidence-based management strategies.
References
Mitrakos, A., Kekou, K., Tilemis, F.-N., et al. (2024). Nablus mask-like facial syndrome: Report of an atypical case with 8q21.3–q22.1 deletion. American Journal of Medical Genetics Part A, 194(12), e63826. https://doi.org/10.1002/ajmg.a.63826
Allanson, J., et al. (2012). Nablus mask-like facial syndrome: Deletion of chromosome 8q22.1 is necessary but not sufficient to cause the phenotype. American Journal of Medical Genetics Part A, 158A(9), 2091–2099. https://doi.org/10.1002/ajmg.a.35446

引用文献
- Mitrakos, A., Kekou, K., Tilemis, F. ‐N., Svingou, M., Papadimas, G., Sofocleous, C., Traeger‐Synodinos, J., & Tzetis, M. (2024). Nablus mask‐like facial syndrome: Report of an atypical case with 8q21.3–q22.1 deletion. American Journal of Medical Genetics Part A, 194(12), e63826. https://doi.org/10.1002/ajmg.a.63826
- Allanson, J., Smith, A., Hare, H., Albrecht, B., Bijlsma, E., Dallapiccola, B., Donti, E., Fitzpatrick, D., Isidor, B., Lachlan, K., Le Caignec, C., Prontera, P., Raas‐Rothschild, A., Rogaia, D., Van Bon, B., Aradhya, S., Crocker, S. F., Jarinova, O., McGowan‐Jordan, J., … Fagerberg, C. R. (2012). Nablus mask‐like facial syndrome: Deletion of chromosome 8q22.1 is necessary but not sufficient to cause the phenotype. American Journal of Medical Genetics Part A, 158A(9), 2091–2099. https://doi.org/10.1002/ajmg.a.35446
- Orphanet. (Last updated October 2010). 8q22.1 microdeletion syndrome. Reviewed by Dr Nicole MORICHON-DELVALLEZ. Retrieved from LINK
- Online Mendelian Inheritance in Man. (Last updated July 2010 by Marla J. F. O’Neill). Retreived from https://omim.org/entry/608156
- Raas-Rothschild, Annick, et al. ‘The 8q22.1 Microdeletion Syndrome or Nablus Mask-like Facial Syndrome: Report on Two Patients and Review of the Literature’. European Journal of Medical Genetics, vol. 52, no. 2–3, Mar. 2009, pp. 140–44. DOI.org (Crossref), https://doi.org/10.1016/j.ejmg.2009.03.011.
- Perez, G., Barber, G. P., Benet-Pages, A., Casper, J., Clawson, H., Diekhans, M., Fischer, C., Gonzalez, J. N., Hinrichs, A. S., Lee, C. M., Nassar, L. R., Raney, B. J., Speir, M. L., van Baren, M. J., Vaske, C. J., Haussler, D., Kent, W. J., & Haeussler, M. (2024). The UCSC Genome Browser database: 2025 update. Nucleic Acids Research, gkae974. https://doi.org/10.1093/nar/gkae974
- Harrison, P. W., Amode, M. R., Austine-Orimoloye, O., Azov, A. G., Barba, M., Barnes, I., Becker, A., Bennett, R., Berry, A., Bhai, J., Bhurji, S. K., Boddu, S., Branco Lins, P. R., Brooks, L., Budhanuru Ramaraju, S., Campbell, L. I., Carbajo Martinez, M., Charkhchi, M., Chougule, K., … Yates, A. D. (2024). Ensembl 2024. Nucleic Acids Research, 52(D1), D891–D899. https://doi.org/10.1093/nar/gkad1049
日本皮膚科学会 皮膚科専門医/日本医師会 産業医/東京衛生検査所 指導監督医
この記事は、 ヒロクリニックNIPTの編集・監修体制 にもとづき、資格を持つ医師が内容を確認しています。







