

World Class Next Generation NIPT
New users here

Registered users here

24hours reservation available
What is Microdeletion Syndrome (Designated Intractable Disease)?
Microdeletion syndrome is a disease caused by the deletion of genes at specific positions on a chromosome.
As the name suggests, the size of the deletion is small, starting from 500,000 base pairs, and it is said to be caused by deletions of sequences typically ranging from 500,000 to 3,000,000 base pairs. The symptoms and severity of the syndrome are determined by the size and position of the deletion, which can lead to various symptoms including developmental delays such as mental retardation. Additionally, most cases of microdeletion syndrome occur spontaneously and are said to occur regardless of the mother’s age.
In other words, it cannot be said that there is no value in testing for pregnant women of any age, from young to old.
What is the Common DiGeorge Syndrome (Designated Intractable Disease 203)?
DiGeorge Syndrome (Designated Intractable Disease 203) is a genetic condition caused by the deletion of a specific region on chromosome 22. This syndrome is known to cause a wide range of effects, including immune system issues, heart defects, and distinctive facial differences. Despite being a relatively rare condition, it can have serious impacts on affected individuals and their families.
Detection Results from NIPT Testing at Hiro Clinic
Among the 3,322 tests conducted at Hiro Clinic, genetic abnormalities related to DiGeorge Syndrome were identified in 5 cases. This is a higher rate than the general epidemiological data, which estimates the occurrence to be 1 in 4,000 to 6,000 people. At Hiro Clinic, the detection rate is about 1 in 600 for DiGeorge Syndrome (Designated Intractable Disease 203). This underscores the importance of the microdeletion syndrome testing advocated by Hiro Clinic. Especially for pregnant women and their families considered to be at high genetic risk, this test provides crucial information, enabling early intervention and preparation.
Microdeletion Syndromes That Can Be Tested with Hiro Clinic NIPT
DiGeorge Syndrome (Designated Intractable Disease 203) is said to be the second most common after Down syndrome among the surviving population. This is believed to be related to its relatively good life prognosis. The following four types of microdeletion syndromes, including DiGeorge Syndrome, can be tested with Hiro Clinic NIPT. All tests are conducted domestically. Currently, due to the small number of samples for microdeletion, positive scores are not provided.
| Case Name | DiGeorge Syndrome | 1p36 Deletion Syndrome | Smith-Magenis Syndrome | Wolf-Hirschhorn Syndrome |
|---|---|---|---|---|
| Affected Region | 22q11.2 | 1p36 | 17p11.2 | 4p16.3 |
| Highest Frequency | 1/2000 | 1/5000 | 1/15000 | 1/50000 |
| Lowest Frequency | 1/6000 | 1/10000 | 1/25000 | 1/96000 |
Reasons Why the Premium Plan is Superior.
The Premium Plan’s high accuracy in detecting microdeletion syndromes sets it apart from other testing companies. Let’s explain the detection of DiGeorge syndrome, which is considered one of the most difficult to detect. In the Premium Plan, more than 80% of the regions prone to deletion (3Mb) in DiGeorge syndrome are read at a depth of over 100x. In comparison, the Illumina overseas test reads at a maximum of approximately 3x (estimated value). The difference in depth directly impacts the accuracy of the test. While standard sequencing typically requires a depth of 30x or more, our plan offers over 100x depth. This level of depth leads to a significant increase in accuracy. This is why the Premium Plan is highly recommended.
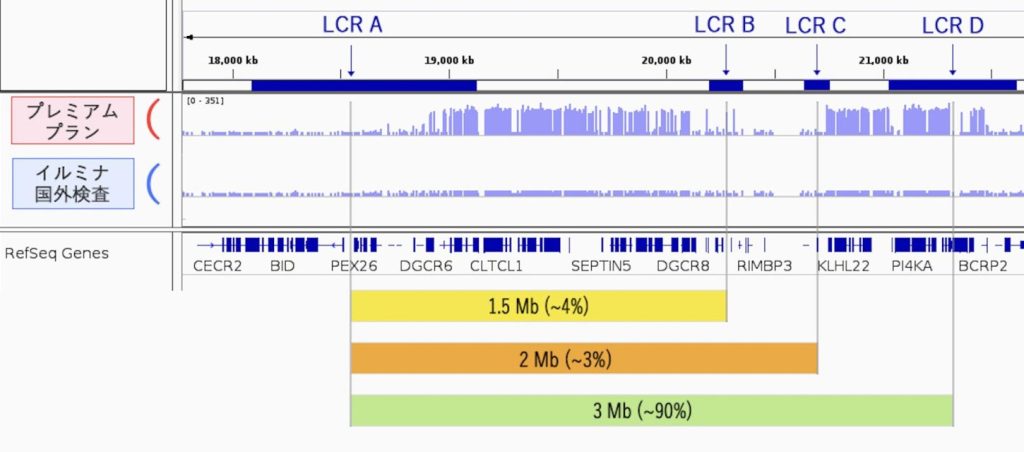
Nearly 90% of DiGeorge syndrome cases involve deletions in the lower green region. The remaining yellow and orange cases are much lower, at 4% and 3%, respectively. It is known that many cases involve deletions of less than 3Mb. Comparing the Premium Plan (Medicover method) with the Illumina method (overseas testing) for this region shows a significant difference in the sequencing depth. The height of the blue bar graph represents the depth of sequencing. The longer bars indicate a depth of over 100X, while the shorter bars indicate 1X. The overseas tests read more deeply in this region than usual, but still only up to about 3X. Normally, they read at about 0.3X, so they are making an effort. The kit used for the entire genome is designed to read broadly but not deeply. Therefore, it is not suitable for detecting such fine deletions.
As explained below, in Illumina overseas tests, if the FF (Fetal Fraction) is below 10%, positive results can turn out to be negative.
Testing Performance at Hiro Clinic
At Hiro Clinic, which has conducted over 56,000 NIPT (Non-Invasive Prenatal Testing) tests, 4,543 individuals have been tested for microdeletion syndromes.
Among the 4,543 individuals, one person received a definitive positive result for DiGeorge syndrome, confirmed by invasive testing. Additionally, among the five inconclusive cases, two underwent amniocentesis, revealing one case of 22q11.2 duplication and another of Emanuel syndrome. The case diagnosed with Emanuel syndrome was identified as 47,XY,+der(22)t(11;22)(q23.3;q11.2) through amniocentesis, indicating a translocation between chromosome 11 at position q23.3 and chromosome 22 at position q11.2. Although the DiGeorge test aims to detect deletions at 22q11.2, abnormalities were detected due to the translocation at this site. This demonstrates that Hiro Clinic’s NIPT can detect abnormalities related not only to deletions but also duplications and translocations. The remaining three individuals have not provided follow-up reports post-testing. Furthermore, out of the five individuals considered highly likely to test positive (borderline), two were later confirmed negative through amniocentesis, while the remaining three did not undergo the test.
DiGeorge syndrome is estimated to occur in approximately 1 in 4,000 to 6,000 people in the general population, caused by a microdeletion on chromosome 22. Through microdeletion syndrome testing, abnormalities in the same regions associated with microdeletion syndromes can also be discovered. To date, at least 3 out of 4,543 individuals have had duplications or deletions detected in the 22q11.2 region through invasive testing. This table will be updated as data from individuals who have not undergone invasive testing becomes available.
| NIPT Test | Amniocentesis Positive | Amniocentesis Negative | Not Performed | |
|---|---|---|---|---|
| Positive | 1 | 1 | 0 | 0 |
| Highly Likely Positive | 6 | 0 | 2 | 4 |
| Inconclusive | 5 | 2 | 0 | 3 |
For reference, Hiro Clinic previously conducted 1,391 Sendout tests with Illumina (Verinata), and all results were negative. These 1,391 tests all included microdeletion syndrome screening.
| DiGeorge Syndrome | 1p36 Syndrome | Cri-du-chat Syndrome | Wolf-Hirschhorn Syndrome | Angelman Syndrome | |
| Positive Cases | 0 cases | 0 cases | 0 cases | 0 cases | 0 cases |
The reason for this is that Illumina’s microdeletion test cannot detect deletions smaller than 3Mb in patients with an FF (fetal fraction) below 10%. (Quoted from “Non-invasive prenatal testing (NIPT) by low coverage genomic sequencing: Detection limits of screened chromosomal microdeletions.”) Since approximately 43% of pregnant women have an FF of less than 10%, there is a high possibility of false negatives in microdeletion tests for DiGeorge syndrome. Patients who previously underwent Verinata testing (Illumina overseas testing) that met these conditions are recommended to be retested using the Medicover method.
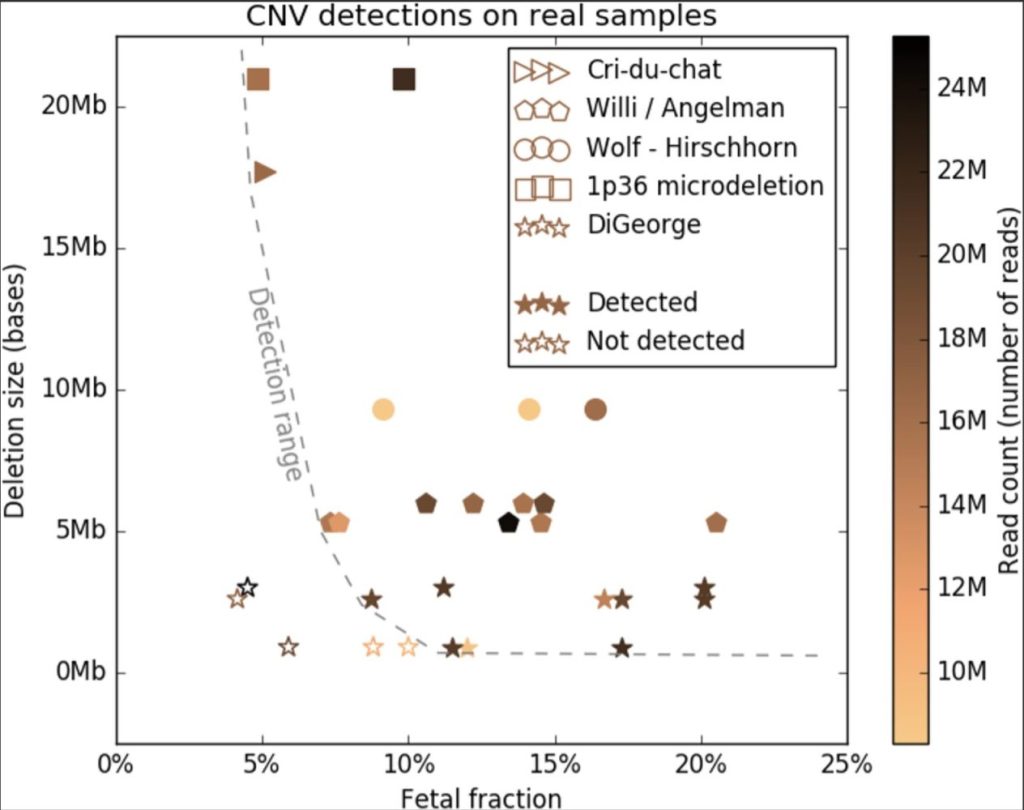
In DiGeorge syndrome, ☆ represents cases that are actually positive but were diagnosed as negative. ★ represents cases correctly diagnosed as DiGeorge syndrome. The vertical axis shows the deletion range. Many stars are located below 3Mb, as about 90% of DiGeorge syndrome cases occur with deletions smaller than 3Mb. The dashed curve represents the detection limit. Cases below this line are false negatives, meaning they should have been detected as positive but were not. The five ☆ in the lower left corner are such cases. Out of 14 cases, 5 are false negatives, resulting in a sensitivity of 71.4%.
In other words, in Illumina overseas tests (not conducted by our company), if the FF (Fetal Fraction) is below 10%, positive results can turn out to be negative.

The distribution of FF (fetal fraction) at Hiro Clinic is as shown above. The proportion of FF below 10% is 43.7% (as of June 2024). This means that nearly half of the individuals have an FF below 10%, resulting in a high possibility of false negatives for DiGeorge syndrome in their test results.
Overview and Symptoms of DiGeorge Syndrome
DiGeorge Syndrome is a genetic disorder caused by the deletion of specific genes. This syndrome can cause a variety of symptoms, including hypoplasia of the thymus and parathyroid glands, congenital cardiovascular abnormalities, and distinctive facial features. Additionally, it is characterized by immune system issues, recurrent infections, and speech difficulties due to submucosal cleft palate.
Overview and Symptoms of Emanuel Syndrome
The phenomenon where parts of chromosomes are exchanged with parts of other chromosomes is called a translocation chromosome. Due to this phenomenon, carriers of the translocation have an increased risk of miscarriage or infertility when having children. Specifically, translocation between chromosomes 11 and 22 can lead to Emanuel Syndrome. This syndrome is diagnosed through specific genetic tests and causes severe congenital abnormalities such as heart defects, cleft palate, imperforate anus, and kidney malformations.
Overview and Symptoms of 22q11.2 Microduplication Syndrome
22q11.2 Microduplication Syndrome occurs due to the duplication of a part of chromosome 22, with 80% of patients exhibiting congenital heart defects. Tetralogy of Fallot is particularly representative, which includes ventricular septal defect and overriding aorta. Cardiovascular diseases significantly affect life prognosis, and a variety of other clinical symptoms are also observed.
| Survey Period | June 2020 – November 2023 | April 2023 – March 2024 |
|---|---|---|
| Survey Organization (Conducted by) |
Tokyo Health Laboratory | |
| Survey Subjects | Individuals aged 19 to 51 who underwent NIPT (Non-Invasive Prenatal Testing) at our clinic | |
| Valid Responses (Sample Size) |
Approximately 56,000 cases | 4,543 cases |
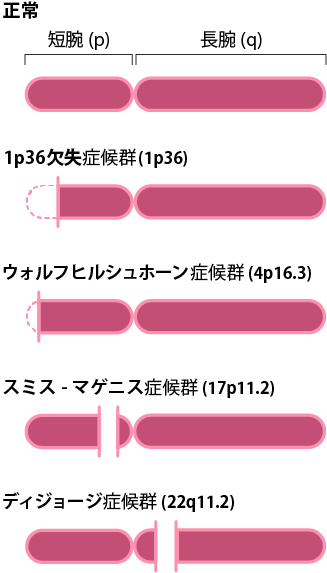
Deletion Sites of the Four Microdeletion Syndromes
The four microdeletion syndromes are caused by deletions in the “long arm of chromosome 22,” “short arm of chromosome 1,” “short arm of chromosome 17,” and “short arm of chromosome 4.” The first number in the affected region indicates the chromosome number, and the subsequent “p” denotes the short arm while “q” denotes the long arm. The short arm refers to the upper part of the chromosome, and the long arm refers to the lower part. The following number indicates the position counted from the centromere.

If Positive, Amniocentesis is Recommended
If the test result is positive, we strongly recommend undergoing amniocentesis. After amniocentesis, the amniotic fluid needs to be subjected to microarray or exome analysis.
Currently, there are few domestic laboratories that perform this test. If you wish to proceed with this analysis and confirm the condition, please consult our clinic. We can refer you to a laboratory.
The Hiro Clinic NIPT plans that include microdeletion syndrome testing are the Premium Plan AM, Premium Plan BM, Premium Plan GM, Premium Plan FM, Premium Plan GM+, and Premium Plan FM+. For more details, please check the test plan page through the button below. Please take a moment to read it.

